
Advances in Applied Psychology, Vol. 1, No. 1, August 2015 Publish Date: Jul. 16, 2015 Pages: 6-9
Prevalence of Functional Disabilities and Sources of Care Provided for Elderly Patients Population in Dubai, UAE
Al Yousef N. J.1, Hussein H.2, *, Al Faisal W.2, Makhlouf M. M.3, Wasfy A.4
1Preventive Services Department, Primary Health Care Services Sector, Dubai Health Authority, Dubai, UAE
2School and Educational Institutions Health Unit, Health Affairs Department, Primary Health Care Services Sector, Dubai Health Authority, Dubai, UAE
3Community Medicine Residency Training Program, Doha, Qatar
4Statistics and Research Department, Ministry of Health, Dubai, UAE
Abstract
Background: Advancing age often goes hand in hand with a loss of autonomy, aggravated by the presence of multiple diseases and a condition of social isolation. Physically, there are changes which take place in human beings; bones become depreciated and osteoporosis appears, muscles degenerate, fat is redistributed and accumulated in specific parts of body such as the waist, and attitudes restructure. Objectives: To study the prevalence of functional disabilities among elderly patient populations and the source of elderly care provided in Dubai, UAE. Methodology: A cross sectional approach was utilized. It was conducted in Primary Health Care centres affiliated to Dubai Health Authority; including family, and geriatric clinics which provide elderly care. The minimum sample size required is 384. Stratified random sample with proportional allocation was utilized. The stratification was based upon the two medical regions of DHA (Deira and Burr Dubai), and clinic type (Geriatric, and Family clinics). Structured standard interview questionnaire was used. Results: 27.5% of elderly patients were partially or completely dependent in 3 functions or more according to Katz index of activities of daily living (Bathing, dressing toileting, transfer, continence and feeding) while the remaining 72.5% were either totally independent or dependent in one or two functions. All elderly patients mentioned that PHC/DHA is the usual source of care (99.2%). Hospital/DHA was the second source of care by males, females and overall (59.3%, 62.2% and 60.9% respectively). More elderly males (15%) as compared to only 6.5% of females claimed that seeking for care abroad was the usual source of care. Conclusions: It is concluded that functional disabilities among elderly patient population is quite high and relevant to the nature of function, most of the elderly patient seeking care service at governmental PHC facilities followed Governmental hospitals. Recommendations: Proper designing of the new PHC centers, and manipulating the already present ones to be more age-friendly by assuring easy accessibility, providing enough parking areas and devoting some of them to elderly, posters (educational posters) used in the center, and number of bathrooms and other facilities.
Keywords
Functional Disabilities, Source of Care, Elderly Patients Dubai
Received: June 3, 2015
Accepted: June 12, 2015
Published online: July 15, 2015
@ 2015 The Authors. Published by American Institute of Science. This Open Access article is under the CC BY-NC license. http://creativecommons.org/licenses/by-nc/4.0/
1. Introduction
Advancing age often goes hand in hand with a loss of autonomy, aggravated by the presence of multiple diseases and a condition of social isolation.(1)Physically, there are changes which take place in human beings; bones become depreciated and osteoporosis appears, muscles degenerate, fat is redistributed and accumulated in specific parts of body such as the waist, and attitudes restructure.(2) Degeneration of cartilaginous tissues, fibrosis and decreased elasticity lead to tightening of joints, and tendency toward osteoarthritis. Cognitive ability is crucial to the capacity to live independently; as the neurons die with diminishing reserve which lead to overall decreases in cognitive function, reduced short term memory, decreased retrieval ability, interrupted and less deep sleep. It also leads to reduced pain, touch, temperature, and vibration sensations and reduced postural control and balance. As human ages, the senses (vision, hearing, taste, smell, touch) may become less acute. The most dramatic sensory changes with age affect vision and hearing but all the senses can be affected by aging.(3) These changes reduce vitality and compatibility of aged people with sudden and somehow unpredictable circumstances and make it difficult for the elderly to readjust to new conditions. Therefore, health needs of aged people are defined differently from those of other age groups.(4)
As the population ages the elderly will come to face certain health states and conditions, although not necessarily unique to the older population, nevertheless have a significant impact on their overall health status. Some of these conditions will result in people becoming more dependants on others for help in performing everyday tasks. The health problems that many elderly people are likely to face are chronic in nature and result in disability and dependency on activities of daily living (ADLs) and instrumental activities of daily living (IADLs).(5) Functional ability is usually expressed through activities of daily living. These activities are either sociable which demonstrates how the person relates to the outside world in leisure and social activities (e.g. going to cinema, visiting friends), or domestic as the elderly abilities to keeps the household going (e.g. cooking, cleaning, laundering, attending to household repair, keeping the house safe). It may be also personal as the elderlys capacity to attend the personal needs (e.g. bathing, dressing, toileting). The convention is to use the term ADLs to cover personal tasks and IADLs to cover household tasks and sociability.(6)
People with age 65 and over account for a far larger share of all those with disabilities (34%) than the total population (12%). They make up an even larger percentage (43%) of those with sever disabilities (US bureau of the census, 1996).(7) A study done in USA, 1992 (5) reported that the percentage of elderly requiring assistance with ADLs increases with age from 2.3% in the 65 to 69 age group to 20% in the 85+ age group. On the other hand the percentage of those needing help with IADLs was higher, with 5% in the 65 to 69 age group needing assistance and 22.3% of those in the 85+ age group requiring help. In this study disability was more prevalent among elderly women than among elderly men (32.9% vs. 22.8%).
Functional disability has numerous implications for public health, including increased demand for health care as visits to physicians and other health practitioners, therapeutic regimens and surgical procedures, dependency on equipment or other people, activity accommodations, hospital stays, nursing home residence, and death.(8) Other implications on reduced quality of life as functional limitation is associated with loss of independence and with increased need for both formal and informal care.(9) Also increased cost of care is one of the implications of functional disability, the total median health care costs per year increased as the number of functional disability increased.(10)
Disability-free life expectancy measures disability by looking at reported limitations in day to day activities such as work, school and leisure activities. The General Household Survey has included such questions in certain years for 65+ year olds. More severe disability and dependence can be measured by people’s ability to carry out activities of daily living such as bathing, dressing, and shopping (which can be used to calculate dependency-free life expectancy). Such measures of functional ability are considered to be more independent of social factors than self-reported health.(1l) Data on the disability and limitations status of the elderly are of importance to policymakers, researchers, and service planners to assess service needs.(12)
2. Objectives
To study the prevalence of functional disabilities among elderly patient populations and the source of elderly care provided in Dubai, UAE.
3. Methods
A cross sectional approach was utilized in the present study. The study was conducted in Primary Health Care centres (PHC) affiliated to Dubai Health Authority including family, and geriatric clinics which provide elderly care in all PHC. The participantes were United Arab Emirates elderly (aged 65 years or more), males and females attending the PHC centre of DHA in Dubai during the period of the study. Elderly patients with communication problem, as those with severe hearing impairment, and elderly patients with a previous diagnosis of dementia were excluded from the study. The minimum sample size required is 384. Stratified random sample with proportional allocation was utilized. The stratification was based upon the two medical regions of DHA (Deira&, Burr Dubai), and clinic type (Geriatric, and Family clinics). Structured standard interview questionnaire was used.
4. Results
Figure (1) displays that 27.5% of elderly patients were partially or completely dependent in 3 functions or more according to Katz index13 of activities of daily living (ADL) (Bathing, dressing toileting, transfer, continence and feeding) while the remaining 72.5% were either totally independent or dependent in one or two functions.
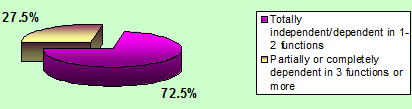
Figure 1. Distribution of elderly utilizing primary health care services at Dubai Health Authority according to ADL scale.
As shown in figure (2), 0nly 1.6% of elderly patients were totally dependent regarding functions of Preparing meals, managing money, shopping, doing housework and using telephone (Instrumental Activities of daily Living scale "IADL").14 Approximately 27% were partially dependent and 71.4% were totally independent regarding IADL scale functions.
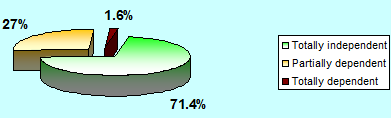
Figure 2. Distribution of elderly utilizing primary health care services at Dubai Health Authority according to IADL scale.
Table 1. Usual source of care among elderly utilizing primary health care services at Dubai Health Authority (n=384).
| Source of care as reported by the elderly in order of frequency | Males N=167 No. (%) | Females N=217 No. (%) | Total N=384 No. (%) | (P-value) |
| PHC/DHA | 166 (99.4) | 215 (99.1) | 381 (99.2) | 0.597 ♯ |
| Hospital/ DHA | 99 (59.3) | 135 (62.2) | 234 (60.9) | 0.560 ♯♯ |
| MOH | 4 (2.4) | 5 (2.3) | 9 (2.3) | 0.605 ♯ |
| Private hospital | 27 (16.2) | 37 (17.1) | 64 (16.7) | 0.818 ♯♯ |
| Abroad | 25 (15.0) | 14 (6.5) | 39 (10.2) | 0.006 ♯♯ |
♯ Fisher exact test
♯♯ Chi-square test
X2= 6.77, P=0.149
From table (1), it is obvious that almost all elderly patients mentioned that PHC/DHA as the usual source of care (99.2%). Hospital/DHA was the second source of care by males, females and overall (59.3%, 62.2% and 60.9% respectively). More elderly males (15%) as compared to only 6.5% of females claimed that seeking for care abroad was the usual source of care. This difference was statistically significant (P<0.01). The overall difference between males and females regarding the usual source of care was not statistically significant (P>0.05).
5. Discussion
Older people are considered a particular group of the population which needs and uses more health services than the rest of the population due to their functional impairments and health status.(15)
Regarding utilization of services, it was found that the average elderly person over 65 years of age in Pakistan, 2009,(16) uses more health care services than nonelderly individuals. More than 50% of the patients were visiting their physicians at least once every two to three months. The present study also revealed that the highest percentage of the elderly were utilizing PHC services less than once/month (66.4%);most of them coming for regular treatment of chronic diseases every 3 months. A previous study conducted in Alexandria 2002, (17)among elderly patients attending different outpatient clinics, found that most of the elderly visit the clinic once or twice/month i.e. 12-24 visit/year. The Asir study (1)demonstrated that their elderly utilized PHC centres fewer times/ year than the younger adult age group. On the other hand, much lower rate of utilization was found among elderly population in Brazil 2007(18), where 72% of them sought and received health care services at least once/6 months.
The present study also revealed that the main reason for choosing of the elderly to their current facility was good quality of services (96.4%) and that the centre is near to their house (91.1%). This may be expected as most of the PHC centres in Dubai had qualified physicians, advanced laboratory services connected to secondary care level hospitals, X- ray services, and specialized clinic as diabetic, dental, ophthalmology and dermatology. Drugs for managing acute and chronic diseases are supplied free of charge to UAE patients. Moreover, PHC centres are distributed to different regions of Dubai, so the elderly can follow up in the nearest of PHC centre. The least reason for utilization was availability of services not provided by others. While in the Alexandria study (17) the main reason for choosing health care facility was that it was free of charge, and the least reason was the quality of care.Similarly Brazil study (18)displayed that their elderly utilized their public clinic than private clinic as the cost of public clinic is lower. This may reflect differences in the socioeconomic levels between the elderly in different countries.
The present study also revealed that almost all the elderly (99.2%) were using the PHC/DHA centre as the usual source of care and half of them were occasionally followed by hospitals of DHA, or private sectors. This may be due to PHC centres provide all the care needed as emergency and follow up. Most of the local nationality elderly have medical records, both in the hospitals with their specialized clinic and at PHC centres. With the adoption of medical electronic system, all physicians can follow their patient investigation, and treatment at both sites. On other hand some PHC centres don’t have specialized clinics as orthopaedic, ENT, and ophthalmology and the elderly my follow at the hospitals. Seeking for care abroad was found to be an alternative to some elderly. A similar situation was found by in Riyadh 2004, (19)where 51% of elderly patients were followed up in Riyadh PHC centre, while 49% were followed up in both PHC and Hospitals. In Alexandria study (17)more than two thirds of the elderly attending geriatric clinic (GC), and pension clinic (PC) as the only source of medical care, while the private facilities was the main alternative for health care.
6. Conclusions
It is concluded that functional disabilities among elderly patient population is quite high and relevant to the nature of function, most of the elderly patient seeking care service at governmental PHC facilities followed Governmental hospitals.
Recommendations
Proper designing of the new PHC centers, and manipulating the already present ones to be more age-friendly by assuring easy accessibility, providing enough parking areas and devoting some of them to elderly, posters (educational posters) used in the center, and number of bathrooms and other facilities.
References
- Mahfouz AA, Alsharif AI, Elgamal MN, Kisha AH. Primary health care services utilization and satisfaction among elderly in Asir region, Saudi Arabia. Eastern Mediterranean health journal. 2004; 10 (3): 365- 371.
- Pourreza A, Khabiri R, Kaldi AR.Health care expenditure and ageing: experiences of developed countries for developing countries such as Iran. Middle East journal of age and ageing, 2007; 4(5): 1-6.
- Besdine RW. Approach to geriatric patient, Geriatric. In: The Merck manuals online medical library.Porter RS, Kaplan JL (editor):18 edition. USA, 2009-2010.
- Pourreza A, Khabiri R, Kaldi A. Health care and ependiture and aging: experience of developed countries for developing countries such as Iran. Middle east journal of age and ageing 2007; 4(5).
- Burke MM, Laramie JA. Demographic: the older population in the United States. In: Primary care of the older adult a multidisciplinary approach. First edition, USA: Mosby 2000: 589-609.
- Kane RA. Social assessment of geriatric patients. In: Geriatric medicine and gerontology. Tallis R, Fillit H, Brocklehurst JC.(editors) fifth edition, England, Churchill Livingstone 1999: 227-234.
- U.S. Census Bureau. Statistical abstract of the United State 1996.
- Griffith L, Raina P, Wu H, Zhu B, Stathokosta L. Population attributable risk for functional disability associated with chronic condition in Canadians older adults.Age and Ageing 2010; 39: 738–745.
- Alves LC, Leite LC, Machado CJ. Factor associated with functional disability of elderly in Brazil: a multilevel analysis. Rev Saude Publica 2010; 44(3):1-10.
- Chan L, Beaver S, MacLehose RF, Jha A, Maciejewski M, Doctor JN. Disability and health care costs in the Medicare population. Arch Phys Med Rehabil 2002;83: 1196-201.
- United Nations. World population ageing: 1950-2050. New York: Population division, department of economic and social affairs, United Nations, 2002.
- Gureje O, Ogunniyi A, Kola L, Afolabi E. Functional disability among elderly Nigerians: results from the Ibadan Study of Ageing. J Am Geriatr Soc. 2006 November ; 54(11): 1784- 1798.
- Nasser R, DoumitJ.Validity and reliability of the Arabic version of Activities of Daily Living (ADL)BMC Geriatrics 2009, 9:11.
- Daniel WW. Biostatistics: A foundation for analysis in the health sciences, 7th Edition, John Wiley & sons, INC, 1999.
- Makhlouf MMEM, Abdel- Kader HZ, Zaghloul AAZ, Ayoub AI. Elderly patients utilization of and satisfaction with medical care provided in outpatient clinics at Alexandria main university hospital and health insurance organization. Bulletin of high institute of public health 2002; 32(1): 55- 74.
- Saleem T, Khalid U, Qidwai W. Geriatric patients expectations of their physicians: findings from a tertiary care hospital in Pakistan. BMC health services research.2009; 9 (205): 1- 10.
- Bos AM. Health care provider choice and utilization among the elderly in a state in Brazil: a structural model. Pan Am J Public Health 2007; 22 (1): 41-50.
- Al Doghether MH, Al Megbil TI.Determinants of prescribing for the elderly in primary health care.Middle eastern journal of age and ageing 2004; 1(1): 1-8.
- Duong DV, Binns CW, Lee AH.Utilization of delivery services at the primary health care level in rural Vietnam. Soc Sci Med 2004 59: 2585–2595.



