
Advances in Applied Psychology, Vol. 1, No. 2, October 2015 Publish Date: Aug. 3, 2015 Pages: 115-119
Health Related Lifestyle Layout Expressed by Adolescents in Dubai
Ali S.1, Al Faisal W.2, *, Hussein H.2, Wasfy A.3
1Preventive Services Department, Primary Health Care Services Sector, Dubai Health Authority, Dubai, UAE
2Health Affairs Department, Primary Health Care Services Sector, Dubai Health Authority, Dubai, UAE
3Statistics and Research Department, Ministry of Health, Dubai, UAE
Abstract
Background: According to WHO, adolescent is a person between the ages 10 and 19 years. Time of adolescence is exceptional for teenagers, as a lot of fundamental changes started in this stage, such changes affecting physical, mental, emotional and social aspects of teenager. Transition from the period of childhood to period of adulthood embraces a lot of stresses encountered by youngster through 3 consecutive stages of adolescence. Objectives: To study the health related life style characteristics of adolescent population in Dubai. Methodology: Cross sectional study was carried out in governmental and private secondary schools of Dubai, UAE, among Secondary school students, grades (10-12), both males and females. Students aged 20 years or more were excluded. The minimum sample size required was 888 students. A Multistage stratified random sampling was carried out. The stratification was based upon region (Bur Dubai and Deira), type of school (governmental and private secondary schools) and sex (males & females). Results: In regard to physical activity, majority of students (45.4%) reported less than one hour exercise in the week. Regarding extra-curricular activities in school, only 31.2% of students have such activities. Presence and practice of hobbies was noted in 92.3% of students. In regard to smoking, it was noticed from the table that 13.3% of students were smokers (either current or past), while 40% of students reported exposure to smoking from others (passive smoking Conclusions: Health related life style among Dubai adolescent population significantly characterized with multiple non healthy behaviors and affected by modern life style deviations.
Keywords
Lifestyle, Adolescents, Dubai
Received: May 24, 2015
Accepted: May 30, 2015
Published online: August 2, 2015
@ 2015 The Authors. Published by American Institute of Science. This Open Access article is under the CC BY-NC license. http://creativecommons.org/licenses/by-nc/4.0/
1. Introduction
Adolescence is a transitional stage of physical and mental human development, generally occurring between puberty and adulthood (age of majority), largely characterized as beginning and ending with the teenage stage.1 According to WHO, adolescent is a person between the ages 10 and 19 years.2 Time of adolescence is exceptional for teenagers, as a lot of fundamental changes started in this stage, such changes affecting physical, mental, emotional and social aspects of teenager.3 Transition from the period of childhood to period of adulthood embraces a lot of stresses encountered by youngster through 3 consecutive stages of adolescence; early, middle and late.4 It is characterized by the rapid physical growth and hormonal development; which is distinctive for males and females, the rapid growth is noticed with the onset of puberty, manifested in bone, muscle, brain, sexual characteristics, and stature. These changes coincide with social and emotional growth, revealed in awareness of others, social consciousness, sense of purpose, personal identity, peer bonding, and intense emotions.5, 6
While this category of population can be seen apparently to have a relatively healthy period of life, they are well-known to be susceptible to variable disorders through their maturation; profoundly in regard to motional maturation, in which they can be vulnerable to mood disorders, in particular to depressive disorders, like major depressive disorder and dysthymic disorder.7 Adolescent depression is a common occurring condition, with reported prevalence in community-residing youth between 0.4% and 8.3% and lifetime prevalence (during adolescence) between 15% and 20%.8
Studies showed that incidence of depressive disorders markedly increases after puberty. At any given time, between 10 to 15 percent of adolescent population have some symptoms of depression, in which five percent of them can meet the criteria to be diagnosed as having major depressive disorder and another three percent as having dysthymic disorder.9
2. Objectives
To study the health related life style characteristics of adolescent population in Dubai.
3. Methodology
Cross sectional study was carried out in governmental and private secondary schools of Dubai, UAE, among secondary school students, grades (10-12), both males and females. Students aged 20years or more were excluded.
Using the computer program EPI INFO "6.04", based on total number of secondary school students of 34299 in Dubai, using 3% degree of precision, an estimated prevalence of 17% 35, 1.5 design effect and 95% confidence limits, the minimum sample size required was 888 students.
A Multistage stratified random sampling was carried out. The stratification was based upon region (Dubai is classified into two main geographic areas Bur Dubai and Deira), type of school (governmental and private secondary schools) and sex (males & females). A list of schools was obtained from knowledge and human development authority.
4. Results
Table (1) clarifies the life style of the study sample of secondary school students. In regard to physical activity, majority of students (45.4%) reported less than one hour exercise in the week. Regarding extra-curricular activities in school, only 31.2% of students have such activities. Presence and practice of hobbies was noted in 92.3% of students. In regard to smoking, it was noticed from the table that 13.3% of students were smokers (either current or past), while 40% of students reported exposure to smoking from others (passive smoking)
Table 1. Distribution of the study sample of Secondary school students according to life style, Dubai 2011.
| Life style | Category | No (n = 1289) | % |
| Physical Activity | no or less than 1 hour per week | 585 | 45.4 |
| 1-2 hours per week | 207 | 16.1 | |
| 3 hours or more per week | 497 | 38.6 | |
| School extra-curricular activities | No | 887 | 68.8 |
| yes | 402 | 31.2 | |
| Hobbies | No | 99 | 7.7 |
| yes | 1190 | 92.3 |
Table (2) describes the exposure of the study sample of secondary school students to physical and verbal abuse through any of their parents. In regards to exposure to physical abuse, 11.8% of students reported such exposure from any of parents. Another exposure to verbal abuse was reported from 26.2% of students.
Table 2. Distribution of secondary school students according to exposure to physical and verbal abuse through their parents, Dubai 2011.
| Physical and Verbal abuse | Category | No (n = 1289) | % |
| physical | No | 1136 | 88.1 |
| Some times | 124 | 9.6 | |
| Frequently | 29 | 2.2 | |
| Verbal | No | 951 | 73.8 |
| Some times | 286 | 22.2 | |
| Frequently | 52 | 4.0 |
Table (3) describes psychological supports among the study sample of secondary school students. Family psychological support was described to be available continuously for 50% of students, whereas 7.6% of students reported absence of family support. Majority as 87.4% of students reported availability of psychological support provided through their close friends
Table 3. Distribution of study sample of secondary school students according to psychological support, Dubai 2011.
| psychological Support | Category | No (n = 1289) | % |
| Family psychological support | No | 98 | 7.6 |
| sometimes | 547 | 42.4 | |
| always | 644 | 50.0 | |
| Close friends psychological support | No | 162 | 12.6 |
| yes | 1127 | 87.4 |
Figure (1) demonstrates the distribution of the study sample of secondary school students according to body mass index. The figure showed that, 31.8% of students are in the categories of overweight and obesity.
Figure (2) describes the distribution of the study sample of secondary school students according to stressful life events. 44.9% of students counted such exposure to death or loss of a relative or close friend in the past year.
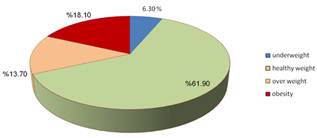
Figure 1. Distribution of the sample of secondary school students according to body mass index, Dubai 2011.
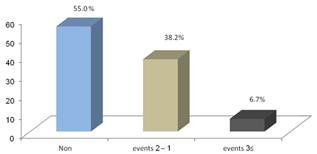
Figure 2. Distribution of the study sample of secondary school students, according to stressful life events (Death or loss of relatives or close friends), Dubai 2011.
5. Discussion
Participants in the study were 1289. They were selected to represent two areas of Dubai and both private as well as governmental schools. Different regional and international studies have recruited different sample sizes. A national Omani study in 2004 has recruited 5409 students,10 in 2005 in KSA, a study conducted on the subject through using 490 students,11 while 1144 students were recruited in similar study in china conducted in 2007.12
Nearly equal numbers were taken from the two main parts of Dubai. This was because of the presence of nearly equal population in these two areas. Private school students are 4 folds more than governmental school students, so they contributed to the selected sample in the same proportion they are in secondary students' population.
The sample was distributed between the ages from 14 to 19 years. Age of adolescents is from 10 to 19 years old according to WHO.2 The age group from 14 to 19 was taken, because of time limitation and simplicity to deal with secondary school adolescents. There was proportionate representation of females and males in the sample. This was because the similar representation in the population. Local students composed one fourth of the sample. This was because Dubai is international city in which a lot of nationalities are there.13
In concern to the sibling’s number, it was noticed that the majority of students have less than 6 siblings. This is an important factor in family constitution that can affect mental status of the students. With large sibling's size there will be lower allocations of care time from both parents. Siblings will be also more likely to grow up in economic adversity, and, as a consequence, they can suffer relatively poor health outcomes.14
Most of students’ parents were educated to the higher level. Most of them were working. The issue can reflect the socio-economic level of families, in which it is of important value in exposing adolescents to circumstances that may participate in mental health development. Studies confirmed the importance of family socio-economic level on maintaining positive conditions that can enhance positive mental status of children and adolescents.15
In majority students, parents are living together. Also the majority of the students were residing with both of their parents. Almost four in five adolescents where satisfied through documenting good relationships with their parents. Such gathering and relationships are good indicators for family dynamics which can affects the growth of adolescent through offering more needed care. In addition, presence of harmonious relationships can ensure the stability of the family and be a protective factor against life stresses.16-18
Disconnection of parents was found in 5% of students, the issue which can lead to disruption of family attachment and impose inverse effects on adolescent's mental status.19,20Almost half of students documented the presence of conflicts between their parents. One from every 20 student was able to observe frequent conflicts between parents. Conflicts are known to be present everywhere, but one of the essential skills that should be practiced by parents is how to hide such conflicts from adolescents, to protect them from any emotional deviation in the future. Studies had recognized possible effects that can lead to forthcoming psychiatric problems among adolescents.21
Regarding relationships of adolescents with their siblings, the majority acknowledged good relationships with their siblings. Positive relationships are essential for maintaining coherence between siblings. Literature showed that positive relationships are essential for maintenance of psychological wellbeing of adolescents especially through provision of support when stressful life events are confronted.22
In school environment, two thirds of students have good relationships with their teachers. Also majority of students documented good relationships with colleagues. Such positive relationships are needed in school, as this environment is the second home for adolescent to grow up. In schools, students need to find support to face changes of adolescents, also they need to find connectedness which help in establishing emotional communications. It was found through research that school environment including (teachers and colleagues) is an important social environment for adolescent mental health. In reference to psychological support, only half of students are offered continuous psychological support from their families. This figure need to be augmented, as psychological support is one of the vital components needed by adolescents through their maturation. In addition, four of every 5 students perceive psychological support from friends. Psychological support from family and friends is essential; this fact has been assured by researches, as they clarify the need for support as guard for mental wellbeing.23, 24
At least one from every ten students is exposed to some form of physical abuse from parents. This exposure is worrying, especially that a percent of 2.2 are exposed frequently. Studies revealed that such exposure to physical abuse is correlated with adverse mental health.25, 26
One quarter of students documented exposure to verbal insults from their parents. Verbal insults are taking to be a form of verbal abuse which leads at the end to emotional abuse of the adolescent. Such exposures are negatively associated with mental health of adolescents. It was documented that emotional abuse is connected with self-worthlessness and hopelessness. Near half of students exposed last year to a stressful life event in the form of death or loss of relative or close friend. It is normal that our life is full of stressful events, which amplify the need for presence of coping strategies that can protect from their possible impacts. It is well known that stressful events can lead to development of psychopathology if not properly managed.27,28
6. Conclusion
Health related life style among Dubai adolescent population significantly characterized with multiple non healthy behaviors and affected by modern life style deviations. Adolescent health program needs to be effectively developed to address the high risky life style layout among adolescent population in Dubai.
References
- Kaczmarek PG, Riva MT. Facilitating Adolescent Optimal Development. The Counseling Psychologist 1996;24(3):400.
- Crawford TV, McGrowder DA, Crawford A. Access to contraception by minors in Jamaica: A public health concern. North Am J Med Sci 2009;1:247-255.
- Taymoori P, Niknami S, Berry T, Ghofranipour F, Kazemnejad A. Application of the health promotion model to predict stages of exercise behaviour in Iranian adolescents. Eastern Mediterranean Health Journal 2009;15(5):1215.
- Neinstein LS. Adolescent health care: a practical guide. : Lippincott Williams & Wilkins; 2007
- Kroger J. Identity development: Adolescence through adulthood. : Sage Publications, Inc; 2007.
- Parker EC. Understanding the process of social identity development in adolescent high school choral singers: A grounded theory 2008.
- Leussis MP, Andersen SL. Is adolescence a sensitive period for depression? Behavioral and neuroanatomical findings from a social stress model. Synapse 2008;62(1):22-30.
- Kubik MY, Lytle LA, Birnbaum AS, Murray DM, Perry CL. Prevalence and correlates of depressive symptoms in young adolescents. American Journal of Health Behaviour 2003;27(5):546-553.
- BHATIA SK, BHATIA SC. Childhood and adolescent depression. Depression 2007;100:53.
- Afifi M, Riyami A, Morsi M, Kharusil H. Depressive symptoms among high school adolescents in Oman. Eastern Mediterranean Health Journal 2006;12:126.
- Abdel-Fattah MM, Asal ARA. Prevalence, symptomatology, and risk factors for depression among high school students in Saudi Arabia. Prevalence 2006.
- Tang J, Yu Y, Du Y, Ma Y, Zhu H, Liu Z. Association between actual weight status, perceived weight and depressive, anxious symptoms in Chinese adolescents: a cross-sectional study. BMC Public Health 2010;10(1):594.
- BRUNSTEIN K. Bullying, depression, and suicidality in adolescents. Journal of the American Academy of Child & Adolescent Psychiatry 2007;46(1):40-49.
- Lawson DW, Mace R. Siblings and childhood mental health: Evidence for a later-born advantage. Soc. Sci. Med. 2010; 70(12): 2061-2069.
- Gabriele B, Heidi M, Gabriele S. The impact of the social environment on children's mental health in a prosperous city: an analysis with data from the city of Munich. BMC Public Health ;10.
- Schoenfelder EN, Sandler IN, Wolchik S, MacKinnon D. Quality of Social Relationships and the Development of Depression in Parentally-Bereaved Youth. Journal of youth and adolescence 2011:1-12.
- Hair EC, Moore KA, Garrett SB, Ling T, Cleveland K. The continued importance of quality parent–adolescent relationships during late adolescence. J. Res. Adolesc. 2008;18(1): 187-200.
- Naevdal F, Thuen F. Residence arrangements and well‐being: A study of Norwegian adolescents. Scand J Psychol 2004;45(5):363-371.
- Aseltine RH. Pathways Linking Parental Divorce With Adolescent Depression. J Health Soc Behav 1996; 37: 133-48.
- Sweeting H, West P, Young R, Der G. Can we explain increases in young people's psychological distress over time? Soc. Sci. Med. 2010.
- Zinzow HM, Ruggiero KJ, Resnick H, Hanson R, Smith D, Saunders B, et al. Prevalence and mental health correlates of witnessed parental and community violence in a national sample of adolescents. Journal of Child Psychology and Psychiatry 2009;50(4):441-450.
- Gass K, Jenkins J, Dunn J. Are sibling relationships protective? A longitudinal study. J.Child Psychol. Psychiatry 2007 02;48(2):167-175
- Afifi M. Depression in adolescents: gender differences in Oman and Egypt. Depression 2006;12(1&2).
- Wight RG, Botticello AL, Aneshensel CS. Socioeconomic context, social support, and adolescent mental health: A multilevel investigation. Journal of youth and adolescence 2006;35(1):109-120.
- Fergusson DM, Boden JM, Horwood LJ. Exposure to childhood sexual and physical abuse and adjustment in early adulthood. Child Abuse Negl 2008;32(6):607-619.
- Peltonen K, Ellonen N, Larsen HB, Helweg-Larsen K. Parental violence and adolescent mental health. Eur Child Adolesc Psychiatry 2010:1-10.
- Timmermans M, van Lier ,P.A.C., Koot HM. The role of stressful events in the development of behavioural and emotional problems from early childhood to late adolescence. Psychol Med 2010 10;40(10):1659-1668.
- Sontag LM, Graber JA, Brooks-Gunn J, Warren MP. Coping with social stress: implications for psychopathology in young adolescent girls. J Abnorm Child Psychol 2008 11;36(8):1159-1174.



