
American Journal of Social Science Research, Vol. 1, No. 4, October 2015 Publish Date: Aug. 12, 2015 Pages: 253-272
Socio-Economic Factors and Orphan Migration in Kisumu District, Kenya
Onganyi O. P.1, *, Ayiemba E.2, Ngala C. O.3
1Department of Social Sciences, Kibabii University College, Bungoma, Kenya
2Department of Geography and Environmental Studies, University of Nairobi, Nairobi, Kenya
3Department of Economics, Masinde Muliro University of Science and Technology, Kakamega, Kenya
Abstract
The growing numbers of AIDS orphans continues to present unprecedented socio-economic challenge to policy makers and institutions that assist them. Orphan migration, though driven by socio-economic necessity, has had untold consequences to spatial and temporal distribution of orphans in Kisumu District. The purpose of this study is to examine the factors in orphan migration in Kisumu District. The study, borrowing heavily from the adult migration and the multiple independent movements of AIDS orphans theoretical perspectives, uses descriptive study design to guide its execution. Pearson’s Chi-square (X2) test was run to test possible association between predisposer background (orphan and care provider) and identified orphan care factors while Logistic Regression model was used to assess the likelihood of orphan care factors driving orphan migration. Qualitative methods using Focus Group Discussions and In-depth Interviews were later employed to get deeper insights on care conditions and socio-economic causes of orphan migration. The study found that geographical disparity of orphans could be explained partly by orphan migration in Kisumu District. It has been demonstrated that care provider background characteristics including sex, place of residence, current marital status, employment status, level of education, and relation to orphan were significantly associated with orphan access to food and clothing, and exposure to stigma, and physical and sexual abuse. Indeed lack of economic and psycho-social support to households that care for orphans were the main cause of orphan mobility. The study recommends that in the short run, the governmental and non-governmental agencies should offer material and technical support to existing orphan care institutions to better care for the orphans. This will help curb high orphan mobility. On the long-term, high structural poverty levels in the region needs to be addressed to enable the community cope better in the management of orphans.
Keywords
Orphan, Orphan Care, Orphan Care Provider, Socio-Economic Factors, Orphan Care Challenges, Orphan Migration
Received: July 6, 2015
Accepted: August 1, 2015
Published online: August 11, 2015
@ 2015 The Authors. Published by American Institute of Science. This Open Access article is under the CC BY-NC license. http://creativecommons.org/licenses/by-nc/4.0/
Contents
1. Introduction 2. Literature Review 2.1. Problems Faced by Orphans 2.2. Orphan Care Challenges 2.3. Orphan Migration 2.4. Theoretical Framework 3. Methodology 3.1. Study Site and Location 3.2. Study Design 3.3. Area Sampling Design 3.4. Population Sampling Design 3.5. Data Collection 3.6. Data Analysis 3.7. Content Analysis 3.8. Study Findings and Discussions 3.9. Demographic Factors 3.10. Socio-Cultural Factors 3.11. Socio-Economic Factors 3.12. Orphan Care Challenges and Orphan Migration 4. Conclusions and Recommendations 4.1. Conclusions 4.2. Recommendations Abbreviations
1. Introduction
The devastating and growing numbers of orphans presents a concern and unprecedented socio-economic challenge to the governments, communities and families of heavily affected countries, and to the agencies and organizations which assist them. Children whose parents have died of AIDS make up the vast majority of this increase (Deininger et al., 2003). World over, the number of orphans aged below 18 years, according to United Nations Children’s Fund (UNICEF) had increased to 16 million by the end of 2009 (UNICEF, 2010), but their geographical distribution at sub-population level remains unknown.
In Kenya, the geography of AIDS epidemic is still at its infancy. A bit has been written on regional and national levels and trends of HIV and AIDS, and orphanhood prevalence and associated health and socio-economic challenges (UNICEF, 2010). Such studies are based mostly on epidemiological surveillance, socio-economic and, demographic and health studies. While it is generally agreed that these regional/national surveys, mostly carried out by international agencies, are a major source of information on orphanhood in the developing countries, their indicators often mask unique socio-economic contexts of orphan care and spatial and temporal variations based on orphan mobility at sub-population level.
Orphan level estimates and trends need not be just based on AIDS prevalence, but should also take into account other population dynamics as well. Migration by orphaned children is one of their adaptation strategies in response to the AIDS crisis. It takes a variety of forms and is becoming an integral part of their everyday living (Ansell et al., 2004). However, despite their engagement in multiple and at times independent movements, there is paucity of information about the socio-economic and demographic context of spatial and temporal relocation of orphans in a cosmopolitan area like Kisumu District. The purpose of this study, therefore, was to examine factors in orphan migration in Kisumu District.
2. Literature Review
2.1. Problems Faced by Orphans
Children whose parents are living with AIDS often experience many negative changes in their lives and can start to suffer neglect, including emotional neglect, long before they are orphaned. Eventually, they suffer the death of their parent(s) and the emotional trauma that results. They may then have to adjust to a new situation, with little or no support, and may suffer exploitation and abuse (Subbarao et al., 2004).
In a study carried out in rural Uganda, high levels of psychological distress were found in children who had been orphaned by AIDS. Anxiety, depression and anger were more found to be common among AIDS orphans than other children. 12 percent of AIDS orphans affirmed that they wished they were dead, compared to 3 percent of other children interviewed (Atwine et al., 2005). These psychological problems can become more severe if a child is forced to separate from their siblings upon becoming orphaned. In some regions, this occurs regularly: a survey in Zambia showed that 56 percent of orphaned children no longer lived with all of their siblings (USAID et al., 2002).
The loss of a parent(s) to AIDS can have serious consequences for a child’s access to necessities such as food, shelter, clothing, security, education and health. In an analysis of orphans and childcare patterns from national surveys of 40 countries, Monasch and Boerma (2004) found that orphans are more likely than non-orphans to live in large, female-headed households where more people are dependent on fewer income earners. This lack of income puts extra pressure on AIDS orphans to contribute financially to the household, in some cases driving them to the streets to work, beg or seek food (Salaam, 2005). The majority of children who have lost a parent continue to live in the care of a surviving parent or family member, but often have to take on the responsibility of doing the housework, looking after siblings and caring for the ill or dying parent(s). Children who have lost one parent to AIDS are often at risk of losing the other parent as well, since HIV may have been transmitted between the couple through sex. In addition, if they do, Deininger et al., (2003) in a Ugandan longitudinal study assert that foster children were highly disadvantaged with respect to health service including vaccination and vitamin A access in Uganda.
Children orphaned by AIDS may miss school enrolment, have their schooling interrupted or perform poorly in school, because of their situation. Expenses such as school fees and uniforms present major barriers, since many orphans’ caregivers cannot afford these costs (UNICEF, 2006). Research carried out locally in Kenya by Mishra and others suggests that children of HIV-positive parents are significantly less likely to attend school than other children (Mishra et al., 2005).
In an earlier study in a rural area near Mutare, Zimbabwe, though the extended family was found to be the principal orphan-care unit, some relatives exploit the children for labour, and fail to meet their educational and medical needs. Only 5 percent of those interviewed felt that there were no differences between themselves and non-orphan children (Foster et al., 1997). Extreme poverty, multiple and mutual exacerbating impact of AIDS including illnesses, draining of dependable family resources and death have been cited as some of the impacts of AIDS in most affected households (Howard et al., 2006).
In an attempt to describe how AIDS has impacted on extended family orphan care arrangements, Nyamukapa et al., (2005) used a combination of both qualitative and quantitative data. They explained the initial absence, followed by emergence of differentials in primary school enrolment between orphans and non-orphans in rural Zimbabwe. The duo found that maternal but not paternal or double orphans have lower primary school completion rates than non-orphans, and that these patterns reflect adaptations and gaps in extended family orphan care arrangements. Low primary school completion among maternal orphans results from lack of support fathers and stepmothers and their ineligibility for welfare assistance due to residence in higher socio-economic status households. However, sustained high levels of primary school completion amongst paternal and double orphans, particularly for girls, result from increased residence in female-headed households and greater access to external resources. These findings indicate that programs should assist maternal orphans and support women’s efforts by reinforcing the roles of extended families and local communities, and by facilitating greater self-sufficiency.
However, with government support, particularly in policy articulation, things could be different. For instance, a longitudinal study in Uganda found a marked increase in the overall school enrolment mainly because of the introduction of free primary education in the country (Deininger et al., 2003). Out of school, AIDS orphans may also miss valuable life - skills and practical knowledge that would have been passed on to them by their parents. Without this knowledge and basic school education, children may be more likely to face social, economic and health problems as they grow up (Salaam, 2005). Lack of such vital livelihood skills may hinder not only their personal enhancement but also their participation in overall development of the country.
Further, children grieving for dying or dead parent(s) are often stigmatized by society through association with AIDS. The distress and isolation experienced by these children, both before and after the death of their parent(s), is strongly exacerbated by the shame, fear, and rejection that often surrounds people affected by AIDS. Because of this stigma, children may be denied access to schooling and health care. Once a parent dies, children may also be denied their inheritance and property. Often children who have lost their parent(s) to AIDS are assumed to be HIV positive themselves, adding to the likelihood that they will face discrimination, which damages their future prospects. Sometimes this occurs because it is assumed that they are infected with HIV and their illnesses are untreatable.
Again, poverty and disease are like tinder and dry wood for raging the fire of the AIDS pandemic. When families are too poor to educate their children, those children will most likely live out their lives in poverty and give birth to a new generation condemned to the same fate. This poverty leaves individuals vulnerable to malnutrition, exploitation and disease (Utan, 2005). Overcoming these twin challenges requires informed decisions based on observed spatio-temporal levels and trends of the orphanhood problem, and massive support to innovative, homegrown approaches that would ensure development based on the principles of equity and sustainability.
2.2. Orphan Care Challenges
In African countries that have already suffered long, severe epidemics, AIDS is generating orphans so quickly that family structures can no longer cope. Traditional systems of taking care of children who lose their parents, for whatever reason, have been in place throughout sub-Saharan Africa for generations. In fact, it has traditionally been said that there is no such thing as an orphan in most African communities.
Traditional safety nets are, however, unraveling as increasing numbers of adults die from HIV-related illnesses. Families and communities can barely fend for themselves, let alone take care of orphans. Typically, half of all people with HIV become infected before they are aged 25 years, developing AIDS and dying by the time they are aged 35 years, leaving behind a generation of children to be raised by their grandparents, other adult relatives or left on their own in child-headed households or even in street life. The demand for care and support is simply overwhelming in many areas. Such demand has strained traditional coping strategies. A number of strategies have emerged to provide this care and support (Drew et al., 1998).
In a study carried out by Cattel (1993), it was observed that though appreciated as a source of pride and self-respect by the elderly, assuming parental responsibilities for the orphans can be burdensome to them. Moreover, when households are stretched with grief, care for the sick, depleted resources and intensified poverty beyond imagination, as in the case of AIDS-affected households, young people’s dependence becomes a terrible liability, not merely the natural order of things (Lusk et al., 2003). Extreme poverty, multiple and mutual exacerbating impact of AIDS including illnesses, death and drain of socio-economic livelihoods have been cited in most affected households.
To explore barriers and possible incentives to orphan care, Howard et al., (2006) conducted a quantitative cross-sectional survey in rural eastern Zimbabwe where 371 adults were caring for children. This included 212 caring for total orphans. They were asked about their well-being, needs, resources, and perceptions and experiences of orphan care. It was found, among other things, that foster caregivers are disproportionately female, older, poor, and without a spouse. Financial, physical, and emotional stress levels were high among current and potential fosterers. They concluded that incentives for sustainable orphan care should focus on financial assistance, starting with free schooling, and development of community mechanisms to identify and support children in need, to evaluate and strengthen families’ capacity to provide orphan care, and to initiate and support placement outside the family when necessary.
In another study by UNICEF in Zimbabwe about community response to care for orphans, it indicated that compared to institutionalization, community based care was more preferred. This was because it kept children in a familiar social, cultural and ethnic environment. It reduced their stress. The crucial role played by the extended families came out clearly; out of 11,514 orphans needing protection, over 11,000 of them were being cared for by relatives living in the same community (UNICEF, 1999).
Lee (2000), in his evaluation of one community based orphan care program in Zimbabwe, concluded that the program was low cost and that evidence from children and caregivers suggested that it was cost-effective. A study by UNICEF in Malawi on community based orphan assistance, showed the model to be culturally accepted and supported. It targeted most orphans and their family members through a right based approach. The model was also found to be flexible, responsive to orphan needs and gave them a chance to participate in issues affecting them (UNICEF, 1998).
On the other hand, institutions, though popular, have been found to be very expensive to run, have limited capacity, cater mainly for physical needs and may encourage dependency. Drew et al., (1998) argue that community-based orphan support programs that use volunteers to visit the neediest children have the potential to complement existing coping mechanisms in a cost-effective manner. Through a program operating in four rural sites in Manicaland in Zimbabwe, 88 volunteers made 9,634 visits to 3,192 orphans in a six - month period in 1996. The total cost of this program in 1996, was US$ 26,000 ($1.5 per visit), 51 percent of which was spent within the affected communities (Drew et al., 1998). In a cost-effective analysis study of orphans in Kenya carried out in Migori District; Owiti (2004) found out that institutional orphanages provide high quality care for orphans and vulnerable children. Conversely, they, among other factors, employ the most expensive structures, hence are the least cost effective. It is not clear whether either solution replaced the services originally delivered by the parents of the orphans.
In an analysis of the Ugandan orphanhood experience, Deininger et al., (2003) assert that foster care has been particularly dramatic for children below school age where, during 1992-2000, the share of foster children increased from 10 to almost 20 percent, with an even stronger increase in the northern part of the country (from 7.2 to 19.3 percent). With almost every fifth child not living with its biological parents, the share of households who have at least a foster child has also increased from about 5 percent in 1992 to 15 percent in 2000. On analyzing the broader macroeconomic consequences of this practice, the trio found out that those households who had to accommodate an orphan invested significantly less than those who did not. This suggests that shocks of this type draw resources away from economically productive pursuits and thus reduce a household’s income generating capacity in the end.
2.3. Orphan Migration
AIDS’ effect on family livelihood through prolonged illness and/or death often induce mobility among surviving family members. This area now receives a lot of research attention as a survival strategy. Some strategies of coping adopted by extended families may have negative impacts on children in households indirectly affected by AIDS, thus enlarging the number of children affected (Ntozi, 1997). For example, children may see their standard of living deteriorate when cousins come to live with them following the death of an aunt or uncle. These ‘other vulnerable children’ experience a reduction in their quality of life and an erosion of the opportunities available for fulfilling their rights.
Changes in the composition of households through migration of family members is an important mechanism by which extended families cope with the economic and childcare need consequences of HIV and AIDS. In a study based in Uganda, Ntozi (1997) argued that urban-rural migration occurs as a result of the ‘going-home-to-die’ phenomenon, whilst rural-urban migration occurs as widows and widowers move to towns to seek work or remarriage. More than one half of young widows and one quarter of young widowers less than 35 years in Uganda moved from the household of their late spouse to earn money or for remarriage (Ntozi, 1997). Similarly, in southern African countries that have experienced a high degree of forced family dispersal, strategies for dealing with AIDS commonly involve splitting children or young people into distant locations, to oscillate subsequently between their own household and that of their extended families (Ansell et al., 2004). In other words, orphaned children move back-and-forth between different ecosystems as their material and social fortunes change.
To study mortality, migration and dissolution of households in northern KwaZulu Natal, South Africa, Hosegood et al., (2003) carried out a large, longitudinal study that found that children households affected by AIDS are more likely to move. Visiting over 10,000 households over the course of the year 2000, they found that children in households where an adult had died from AIDS were 60 percent more likely to migrate that same year. This was especially so if it was the child’s mother or father who had died. Looking at child migration by gender and age, a household survey in Kenya (Yamano et al., 2004) found that older daughters commonly leave the household after the death of a male head, while younger children were more likely to leave the household after the death of a female head.
The type of parental death, therefore, largely influences whether changes in residence and caregiver occur: for example, paternal orphans have been found to be more likely to continue residing with their surviving parent than maternal orphans (Nyamukapa et al., 2005; UNICEF 2003). Orphanhood may also affect the socio-economic status of orphans. School attendance among orphans would differ depending on whether or not the parent(s) who died were the primary breadwinners of the household (Nyamukapa et al., 2005).
Urassa et al., 2001, in a cohort study in Tanzania found that the mobility of household members was high before and after a death, especially when the head of a household died. All members moved out of the household (irrespective of cause of death) in 44 percent of households in which the head died. In contrast, none of the deaths on non-head adult members led to household dissolution. In Eastern Zimbabwe, Mutangadura et al., (2001) noted that the majority (65 percent) of households where deceased adult females lived before dying was no longer in existence, in both urban and rural studies.
Further analysis of a cohort based study in Karonga in Malawi by Crampin et al., (2003) examined the impact of AIDS on household structure to assess how spouses and offspring were affected. It was common (73 percent) for households to dissolve following the death of a mother whose HIV-positive husband had already died. The likelihood of dissolution was smaller (34 percent) after the death of a widowed male spouse. This study also found a lower probability that wives of HIV-positive men re-marry after widowhood/separation compared to wives of HIV-negative men (this appeared to be an issue of age rather than stigma). Perhaps, therefore, widows of HIV-positive men were more likely to become heads of households, in an area where female-headed households are traditionally rare.
To explore whether the AIDS epidemic is contributing to the number of street children in southern Africa, Mawoneke et al., (2001) investigated the main factors responsible for increased number of street children in two cities in Zimbabwe. Half the street children in Zimbabwe are orphans, more than twice the proportion of orphans found in the general population. The main factors that led children to the streets were poverty, a desire to handle their own money, ill treatment by guardians, orphanhood, ill treatment by parents, and overcrowding at home. The majority of street children who were double orphans (56 percent) and those who were maternal orphans (59 percent) lived on the streets most of the time. The majority of paternal orphans in the sample (68 percent) and non-orphans (71 percent), however, lived at home or with a guardian. Of the paternal orphans on the street, 59 percent lived with their mother, but only 6 percent of the maternal orphans lived with their fathers (Mawoneke et al., 2001).
2.4. Theoretical Framework
The study borrows from two theoretical perspectives. They include the adult migration and the multiple independent movements of AIDS orphans perspectives. These theoretical perspectives help to unveil theoretical understanding of the selective nature of spatial and temporal AIDS orphan migration in different socio-economic contexts.
Adult labour migration that involves the migration of male heads of households to urban and to rural areas is critical in examining orphan distribution in heavily affected regions. This is particularly the case in most African countries, where a larger proportion of adult migrant workers living in towns away from home have a well-documented high AIDS prevalence (Ghosh, et al., 2004). However, this does not necessarily imply high prevalence of orphanhood there but may lead to rising numbers of orphans in the home village where the families of the infected are located.
Perhaps a strong explanation behind the geographical disparity of orphans is to be found in the migratory activities linked with the survival strategies of the children themselves. According to the multiple independent movements of AIDS orphans perspective, orphans are hard to locate as a group because they are always on the move geographically and between different care giving environments. As a result, orphans not only negotiate their livelihoods and assume new social and economic responsibilities but also autonomously redefine their social and geographical position in their own society, which may include migration to environments perceived to be more secure.
However, it is important to note that the field of HIV and AIDS is relatively new and hence theoretical understanding of the epidemic is still evolving.
3. Methodology
3.1. Study Site and Location
Kisumu District lies in a down warped part of lowland surrounding the Nyanza Gulf, at the tip of which is Kisumu City. It is one of the twelve districts forming what until 2010 was Nyanza Province. The district borders Nyando District to the East, Vihiga District to the North, Nandi District to the Northeast, Siaya District to the Northwest, Bondo District to the West and Lake Victoria to the South. The District lies within longitude 33 20’E and 35 20’E and latitude 0 20’S and 0 50’S. The district covers 918.5 square kilometres and has four administrative divisions (Ministry of Planning, National Development and Vision 2030, 2010).
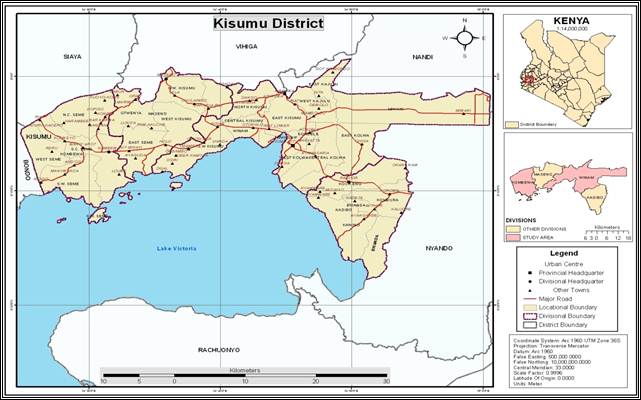
Figure 1. Administrative boundaries of Kisumu District.
Source: Researchers, 2015
The 2009 Kenya Population and Housing Census report, indicated that the district had 618,556 people distributed in the four divisions as follows: Winam (412,323), Maseno (77,554), Kombewa (67,353) and Kadibo (61,326) (GoK., 2010). Winam Division hosts Kisumu City, the provincial headquarters of the former Nyanza Province, Kenya. Figure 1 illustrates the administrative boundaries of Kisumu District.
Geographic position of the study area and its relevance to economic activities, population mobility and spread of HIV and orphanhood is critical in this case. Kisumu City, being the third most populous city in Kenya after Nairobi and Mombasa, and a fast growing urban centre in Nyanza region, is the destination for migrants of both sexes in search of employment within the city. In the city’s neighbourhood, there are a series of large scale agricultural activities including sugarcane in Miwani, Muhoroni, Chemelil and Kibos, and rice in Ahero and Kano irrigation schemes. These plantations and their processing factories attract high migrant populations from everywhere either working directly in the agricultural companies or doing business around the area. Moreover, Kisumu District has a series of fish landing beaches, which also attract many migrant populations interested in the fish industry in the area. Kisumu is strategically located on the major highway to Uganda to the North West, and it has a direct link to Tanzania in the South. For decades, the town has been a major trading link for Uganda and it is an important transit point for travellers throughout East Africa. This rural-urban interface in the context of large and highly mobile population has had and continues to have consequences for high HIV and AIDS related mortality and orphanhood prevalence.
3.2. Study Design
The study uses descriptive study design. Mixed-method approach is employed where quantitative methods including inferential statistics were used to show the link between orphan and care provider background factors and orphan migration. Qualitative methods were later used to get deeper insights on orphan care conditions and predisposer factors in orphan migration.
3.3. Area Sampling Design
Kisumu District had four administrative divisions; Winam, Maseno, Kombewa and Kadibo. The four divisions had twenty four (24) locations half of which (12 locations) were located in Winam Division alone, and four each in the remaining three divisions. For better representation, diversity and rural-urban comparative analysis, therefore, two divisions (Winam-largely urban, and Kombewa-rural) were purposively selected for deeper insight on rural-urban context of causes of orphan migration in the study area.
3.4. Population Sampling Design
The study targeted 420 orphans in primary and secondary schools out of 92,593 orphans in Kisumu District. The study considered orphans under formal institutionalized care and foster care arrangement in Winam and Kombewa Divisions of Kisumu District. Due to ethical considerations, however, only those orphans aged 8-17 years were involved in the study. Care providers both from formal institutionalized and foster care systems, and opinion leaders in the study area were targeted in this study.
A sample saturation approach was used in conducting in-depth interviews (IDIs) among fifty two (52) total orphans aged 8-17 years and seventeen (17) care providers based in informal (13) and formal (4) care and support institutions. In addition, eighteen (18) local opinion and sector leaders were predetermined and purposively selected. Out of the eighteen (18) opinion and sector leaders, six (6) were from relevant government department (2 local gender, children and social development, and 4 provincial administration) officials; eight (8) local community leaders including teachers, retired civil servants; two (2) officials of community service organizations; and two (2) local women and youth groups. Opinion and sector leaders were people who were knowledgeable in orphan care and support issues, either by virtue of working directly with orphans or indirectly by working with agencies operating in the study area to assist orphans in various ways. They were drawn from local members of the community, relevant government officials, community service organizations and local community group representatives. In addition, eight (8) focus group discussion (FGDs) sessions were conducted with orphans in upper primary (standard 4 to 8) and secondary schools (form I to III). A session consisting of ten homogeneous participants, two from each level of schooling per site was considered. FGDs were meant to gain deeper knowledge on crosscutting orphan care related issues.
3.5. Data Collection
To gain deeper insights on orphan care conditions and causes of orphan migration, 420 orphans drawn from primary and secondary schools were interviewed. The study also conducted 87 in-depth interviews (IDIs) consisting of 52 orphans, 17 care providers and 18 key opinion leaders in the study area. The local opinion leaders were particularly targeted because of their wealth of knowledge and experience on socio-economic issues affecting the community like those related to orphan migration. In addition, to gather information on crosscutting issues related to orphan care, 8 FGDs were conducted with orphans in both primary and secondary schools in the study area. Each session consisted of about ten participants and gender equity was ensured.
3.6. Data Analysis
Pearson’s chi-square (X2) test: Chi-square test was run to test possible association between predisposer background (orphan and care provider) factors and orphan care need factors including access to food, shelter, clothing, education, health care, inheritance, time to play, parental love, and exposure to stigma, physical and sexual abuse among others.
Logistic regression: A Logistic regression model was used to assess the likelihood of identified orphan care factors driving orphan migration. Ensminger (1992) argued that internal and external factors interact to influence each other and influence orphan migration. Based on this argument, most important causal relationships were identified, by narrowing the range of relevant theoretical variables and their interactions based on the study context. A Logistic regression was preferred over other regression models because of the categorical nature of the dependent variable. Wuensch (2004) and Hosmer et al., (1989) support this approach when the dependent variable is dichotomous.
(i) Independent (explanatory) intermediate variables
Independent variables were developed through a conceptual causal relationship between dependent (orphan migration) and intermediate independent orphan care challenge variables that were found important for the study.
(ii) Dependent variable (response)
Orphan migration as a dependent variable was measured considering whether the orphan had changed place of residence (migrated) or not since the parent(s) died. The following causal links were developed;
Orphan migration = f (food, shelter, clothing, education, health care, inheritance, stigma, physical abuse, sexual abuse, parental love, time to play).
From this causal relationship, logistic model was developed to gauge statistically significant factors driving orphan migration. The logistic model used was in the form;
![]() =
= ![]() +
+ ![]() +
+ ![]()
![]() + err
+ err
Where;
Yi = depended variable indicating orphan migration.
X1 . . .Xn = independent intermediate variables.
3.7. Content Analysis
Qualitative data was analyzed using content analysis approach to make sense of the texts which were generated in the IDI scripts and FGD transcripts. Silverman (2006) has advocated for this approach. It recommends establishing a set of categories, and then counting the number of instances that fall into each category. The study proceeded by coding respondents’ answers into different sets of categories. Three concurrent data processing activity flows as suggested by Miles et al., (1998) was then followed: data reduction (simplifying and abstracting data), data display (assembling information as to permit drawing conclusions), and verification and conclusion (giving provisional meanings to regularities, patterns and flows, and testing provisional conclusions). At this stage, the findings were linked to the study objectives, assumptions and theoretical framework, and existing literature.
Data presentation techniques like tables and maps were used to illustrate variations in orphan care and orphan migration in Kisumu District. The two data sets were triangulated for validation purposes.
3.8. Study Findings and Discussions
3.8.1. Orphan Background Characteristics and Orphan Care Challenge
When Pearson’s Chi-square (X2) test statistic was run to test possible association between predisposer orphan background factors and orphan care need factors including access to food, shelter, clothing, education, health care, inheritance, time to play, parental love, and exposure to stigma, physical and sexual abuse among others, it was established that some orphan care challenges could be associated with orphans’ own background characteristics. For instance, an orphan’s level of education was significantly associated with orphan access to shelter (X2 = 7.989; df = 1 and p < 0.05), and clothing (X2 = 7.088; df = 1 and p < 0.05) (see Table 1). That is, those in secondary schools were more likely to report problems related to shelter and clothing than their primary school counterparts. The following assertions by affected orphan respondents further explain the linkage.
There are so many challenges that they (girls) face. You may find a girl being left with the young ones to take care of all the time (don’t go to school); cook for them and this may force them to get into early marriage. They are so much stressed when they cannot get support from their (other) relatives or neighbours (A girl of15 years, Form 1, Winam Division).
Boys are forced to do a lot of work like being hired for labor, while the care provider takes all the money (A girl of14 years, class 7, Winam Division).
Since level of education is chiefly a function of age, it was possible to link this finding to demand for a higher level needs beyond, for instance food among older orphans as explained in Maslow’s hierarchy of needs. As Maslow's theory suggests, most basic level of needs must be met before an individual will strongly desire (or focus motivation upon) the secondary or higher level needs. Clothing and shelter rank higher (safety need) compared to food (physiological need) in the hierarchy of needs. In a related study carried out by Population Council in Kisumu District and other parts of Nyanza, many orphans were reportedly unable to access a range of basic necessities even though there was no significant difference in economic status of households with or without orphans (Population Council, 2007). Despite the fact that lack of shelter affects orphans of almost all ages, older ones in secondary schools were understandably more likely to report lacking such basics compared to their younger counterparts, perhaps, because of differences in their developmental needs with age.
A study carried out among orphans and non-orphans by Population Council in Nyanza, found that lack of loving care by guardians was perhaps the key factor that increases vulnerability and that orphaned girls and especially those who had lost their mothers, were the least likely to feel they had such support (Population Council, 2007). With regard to education, many studies had initially reported that orphans, particularly girl orphans, were more disadvantaged with regard to access to education (UNAIDS, 2008; Ainsworth et al., 2002). In many AIDS affected contexts, orphans are less likely to be enrolled or at their proper educational level than non-orphans of the same age. Double orphans appear to be at the highest risk, and loss of a mother may prove more detrimental than loss of a father (Population Council, 2007).
In a study of orphans in Tanzania, Ainsworth et al., (2002) found that enrolment of large proportions of young children was delayed, while enrolment of older children was maintained. Among the children whose enrolment was most affected at the primary level were children in poor households suffering an adult death, especially the maternal orphans. Makame et al., (2002) found that in a poor neighbourhood of Dar El Salaam (Tanzania), though orphans were less likely to be in school, those in school were attending as regularly as the non-orphans. In a study conducted in eastern Zimbabwe, Nyamukapa et al., (2003) observed that children whose parents had died recently were equally likely to have started school as children of the same age whose parents were alive. As time passed since their mother’s death, children who had lost their mother were less likely to have completed primary school than children who had lost their father or children whose parents were living, suggesting that widowed mothers give higher priority to their children’s education than widowed fathers. Using demographic and health survey (DHS) data from Ghana, Kenya, Niger, United Republic of Tanzania and Zimbabwe, Bicego et al., (2003) found that orphans were less likely than non-orphans to be at their proper educational level, with the effect stronger at younger ages (6-10 years) than older ages (11-14 years). They also found double orphans were at a particular disadvantage.
Table 1. Cross tabulation of selected (statistically significant) orphan background factors against orphan care challenges.
| Orphan background factors | Responses within background factors | |||
| Yes | No | |||
| Number | Percentage | Number | Percentage | |
| Sex of orphan*Food | ||||
| Male | 127 | 58.8 | 89 | 41.2 |
| Female | 155 | 76.0 | 49 | 24.0 |
| Chi-Square = 14.043 | ||||
| degrees of freedom = 1 | ||||
| p value (level of significant)=0.000*** | ||||
| Sex of orphan*Stigma | ||||
| Male | 119 | 55.1 | 97 | 44.9 |
| Female | 134 | 65.7 | 70 | 34.3 |
| Chi-Square = 4.916 | ||||
| degrees of freedom = 1 | ||||
| p value (level of significant) = 0.027* | ||||
| Level of education *Shelter | ||||
| Primary | 179 | 56.8 | 136 | 43.2 |
| Secondary | 76 | 72.4 | 29 | 27.6 |
| Chi-Square = 7.989 | ||||
| degrees of freedom = 1 | ||||
| p value (level of significant) = 0.005** | ||||
| Level of education*clothing | ||||
| Primary | 182 | 57.8 | 133 | 42.2 |
| Secondary | 76 | 72.4 | 29 | 27.6 |
| Chi-Square = 14.341 | ||||
| degrees of freedom = 1 | ||||
| p value (significant level) = 0.000*** | ||||
| Sex of orphan*School attendance | ||||
| Male | 139 | 64.4 | 77 | 66.4 |
| Female | 165 | 80.9 | 39 | 33.6 |
| Chi-Square = 14.341 | ||||
| degrees of freedom = 1 | ||||
| p value (level of significant) = 0.000*** | ||||
| Note: *Cross tabulation; *, **, *** = statistically significant at p < 0.05, 0.01 and 0.001 respectively N=420 | ||||
Source: Researchers, 2015
In recent times, several studies on the impact of orphanhood on education have reached different and at time divergent findings, an indication that some trends about orphanhood and education may be emerging. In Kenya, there is reportedly no significant difference in school enrolment between orphans and no-orphans (UNICEF, 2010). This could be due to the introduction of free primary education policy by the Kenyan government in 2003. A longitudinal study in Uganda also found a marked increase in the overall school enrolment mainly because of the introduction of free primary education in the country (Deininger, et al., 2003).
However, girls were reportedly likely to attend school more irregularly than boys. While gender parity is almost achieved in Kenya with regard to school enrolment of orphans and non-orphans, a distinction should be made between school enrolment and attendance. While Kenya has been praised for almost achieving gender parity in basic education enrolment, orphans, particularly of the girl gender still face major challenges with regard to regular school attendance. According to Population Council, while virtually all orphans (97 percent) were enrolled in school, older female orphans were the least (86 percent) likely to be in school in Nyanza Province (Population Council, 2007).
Further, the qualitative interviews and discussions also established that there were gender differences with regard to orphan challenges and response to such challenges. Lack of adequate orphan care and mistreatment were singled out as the key challenges to most orphans both in rural and in urban areas. Gender differences in response to such challenges emerged. Mistreatment and lack of support in meeting personal and basic needs, and being denied an opportunity to attend school reportedly led to early sexual debut, early pregnancy, child labour, prostitution and early marriage among girls. Girls were singled out by care providers, opinion leaders and the orphans themselves to be more vulnerable when their psychological and personal needs were not met. A report from the World Bank (WB) reported that girls are more likely than boys to be retained at home for domestic work or for care-giving when incomes plummet due to AIDS deaths (World Bank, 2002). A study by UNAIDS also pointed out that prime age-adult deaths cause the removal of children, especially girls, from school (UNAIDS, 2002).
Girl orphans faced increasing cases of physical and sexual abuse with dire consequences to their health and general wellbeing. Unfortunately, numerous cases of abuse go unreported as they were largely linked to care providers and their close relatives. Dawes et al., (2007) reported that all evidence regarding sexual abuse and rape are limited by inadequate reporting and recording, particularly in the developing world. In urban areas, for instance, the study found that relatives particularly the elder children of care providers were the main culprits. In a related finding, Jewkes et al., (2003) carried out a study on the prevalence of domestic violence among orphan samples in South Africa that indicated that there were heightened levels of violence in AIDS affected families. Gregson and others in a study based in eastern Zimbabwe found that orphaned children were more likely to have had sex at younger age than non-orphans. They also observed that female orphans in eastern Zimbabwe had higher teenage pregnancies, STIs and HIV-prevalence than non-orphans (Gregson, et al., 2005). In most cases, they have older sexual partners (Muula, et al., 2003; Oleke, et al., 2007). Lack of loving care by guardians was perhaps the key factor which increased vulnerability and orphaned girls were the least likely to feel they had such support (Population Council, 2007). Girls who had lost their mothers were considerably more likely to have had sex due to lack of love, care and parental guidance from guardians than girls whose mothers were still alive. Orphans were more likely to be given more work and less affection than other children in their households (Population Council, 2007).
On boy orphans, inadequate care was found to be associated with school dropout, child labour/child abuse and early marriage among others. Case et al., 2003; Nyamukupa et al., 2003; Makame 2002 had linked orphan school dropout to child abuse including child labour. Early marriage in some cases reportedly involved young orphaned boys, who in the middle of extreme poverty and lack of any sort of financial and emotional support, were reportedly being lured into widow inheritance for promise of better care and support by widows. Population Council had pointed out, in a study conducted in Nyanza, that boys who had lost their mothers were more vulnerable to early marriage, particularly to young widows (Population Council, 2007). Similar results have been documented by Oleke et al., (2007) and Thurman et al., (2006).
In general, inability to meet to basic needs, including education was reported to be the most critical challenge facing orphans in urban and rural areas. Rampant poverty and lack of sufficient income to meet the basic needs were cited as key factors. Orphans in the foster care arrangement were more likely to experience lack of the basic and particularly psychosocial needs from their care providers. Very few of those orphans based in the modern institutionalized care system (orphanages) complained about these needs after joining the centre. Widespread poverty throughout Nyanza Province was perceived by adults and children to be a major factor putting all children at risk (Population Council, 2007). That inability to meet basic and personal needs, rather than money parse, such as school fees and materials, food, clothing, bending, soap and body/hair oil, was thought to motivate children to engage in transactional sex to be able to meet these needs (Oleke et al., 2007; Population Council, 2007; Muula et al., 2003). UNICEF had affirmed that though the physical needs of orphan such as nutrition and health care appear to be the most urgent, emotional needs of children who have lost a parent (s) should not be forgotten (UNICEF, 2010).
3.8.2. ProviderCharacteristics and Orphan Care Challenge
Pearson’s Chi-square (X2) test statistic was run in the cross-tabulations to test possible association between foster care provider background factors and orphan care need factors including access to food, shelter, clothing, education, health care, inheritance, time to play, parental love, and exposure to stigma, physical and sexual abuse among others (see Table 2). It was established that some orphan care challenges could be associated with some care provider demographic, socio-cultural and socio-economic characteristics.
3.9. Demographic Factors
Sex of care provider was found to be significantly related to sexual abuse experience (X2 = 4.705; df = 1 and p < 0.05) by the orphan (see Table 2). Those orphans living with female care providers were more likely to experience sexual abuse than those living with male care providers. This could probably be explained by the fact that a number of care providers were old, widowed poor female grandparents. In their condition, they are unable to adequately meet the needs of orphans under their care forcing such orphans to engage in risky pursuits to earn a living, a fact that exposes them to sexual abuse. The following statements by orphan discussants captured the challenges facing orphans without proper care in the study area.
The lake region is very dangerous for the orphaned girls because fishermen in exchange for sex give them money. Most of them drop out of school. In many cases, they become pregnant and get HIV. The rate of HIV infection is very high because they do not depend on one man. All these are happening because they lack (proper) care and support (A boy of17 years, class 7, Kombewa Division).
They (care providers) may support you but tell you to go for some casual work to buy things like pens (A boy of15 years, Form 2, Kombewa Division).
In an analysis of orphans and childcare patterns from national surveys of 40 countries, Monasch and Boerma found that orphans are more likely than non-orphans to live in large, female-headed households where more people are dependent on fewer income earners (Monasch et al., 2004). It could also point out to the fact that orphans under the care of old female grandparents are more vulnerable to sexual abuse due to inability (perceived or real) of such old care providers to offer social and physical protection. Additionally, there are many reported cases of widows preying on desperate young orphans for remarriage with promises of good care and support.
Table 2. Cross tabulation of selected (statistically significant) care provider demographic and socio-cultural factors against orphan care challenges.
| Care provider background factors | Responses within background factors | |||
| Demographic | Yes | No | ||
| Number | Percentage | Number | Percentage | |
| Sex of care provider*sexual abuse | ||||
| Male | 34 | 25.0 | 102 | 75.0 |
| Female | 19 | 35.6 | 183 | 64.4 |
| Chi-Square = 4.705 | ||||
| degrees of freedom = 1 | ||||
| p value (significant value) = 0.030* | ||||
| Socio-cultural factors | ||||
| Current marital status*Food | ||||
| Never married | 26 | 86.7 | 4 | 13.3 |
| Married | 180 | 69.8 | 78 | 30.2 |
| Divorced/ separated | 8 | 61.5 | 5 | 38.5 |
| Widow (er) | 68 | 57.1 | 51 | 42.9 |
| Chi-Square = 11.568 | ||||
| degrees of freedom = 3 | ||||
| p value (significant value) = 0.009** | ||||
| Current marital status*parental love | ||||
| Never married | 22 | 73.3 | 8 | 26.7 |
| Married | 151 | 58.5 | 107 | 41.5 |
| Divorced/separated | 5 | 38.5 | 8 | 61.5 |
| Widow(er) | 59 | 49.6 | 60 | 50.4 |
| Chi-square = 7.926 | ||||
| degrees of freedom = 3 | ||||
| p value (significant value) = 0.048* | ||||
| Relation to care provider *Food | ||||
| Paternal grandfather | 6 | 40 | 9 | 60.0 |
| Paternal grandmother | 17 | 34 | 33 | 66.0 |
| Maternal grandfather | 10 | 66.7 | 5 | 33.3 |
| Maternal grandmother | 34 | 75.6 | 11 | 24.4 |
| Paternal uncle/aunt | 60 | 69.8 | 26 | 30.2 |
| Maternal uncle/aunt | 61 | 79.2 | 16 | 20.8 |
| Other relatives/ non-relatives | 94 | 71.2 | 28.8 | 28.8 |
| Chi-Square = 37.701 | ||||
| degrees of freedom = 6 | ||||
| p value (significant value) = 0.000*** | ||||
Source: Researchers, 2015
3.10. Socio-Cultural Factors
Care provider relation to the orphan was significantly related to access to food (X2 = 37.710; df = 6 and p < 0.05); clothing (X2 = 18.835; df = 6 and p < 0.05); education (X2 = 21.770; df = 6 and p < 0.05), and show of parental love (X2 = 14.221; df = 6 and p < 0.05) by the orphan.
In most cases, living with uncle/aunt from either paternal or maternal side of the family was found to be disadvantageous to an orphan with regard to access to most basic care needs (see Table 3). Most uncle and aunties were probably having their own children of similar ages hence a lot of pressure caring for the orphans. Uncles, particularly from the paternal side of the family were singled out for mistreating orphans under their care. They reportedly mistreated the orphans to scare them away so that they could disinherit the orphans of property left behind by their parents. The following statements by affected orphans help put things into perspective.
You may be staying with a brother and his wife mistreats you by giving you too much work that you cannot even study. If you tell him, he will take his wife’s side, it is very painful (A boy of girl of15 years, Form 1, Winam Division)
Paternal relatives are very bad. They would want to take your parent’s property, so they will mistreat you so that you leave the wealth to them (A girl of15 years, Form 1, Kombewa Division)
Both my parents died during the post election violence. During my parents’ burial, my uncle promised to take care of me and he took me to his home after the burial. All was not the same, he started mistreating me. One day, he took me near the lake and left me there, and warned me not to follow him back. I had no place to go to, then that evening one of the fishermen found me and took me to the chief’s camp. I was later taken to Mama Ngina Children’s Home. I am now feeling okay at Mama Ngina (A girl of 12 years, Class 6, Winam Division)
Similarly, Case et al., (2003) investigated the impact of orphanhood on primary school enrolment in 10 sub-Saharan countries between 1992 and 2000. They found that orphans were at a significant risk for lower school enrolment, and that this risk was not explained solely by their relative poverty. Searching for explanations beyond household wealth, the researchers discovered that orphans were less likely to be enrolled in school than non-orphans living in the same household. They proposed that the critical determinant is the nature of the family relationship between the orphan and the decision-making adult in the family or household, consistent with ‘Hamilton’s Rule’. The rule postulates that closeness of biological ties governs investments in children. They found that, as a general pattern, the probability of school enrolment is related to the closeness of the relationship between the child and the household head.
Children living in households headed by non-parental relatives fare worse than those living with parental heads, and those living in households headed by non-relatives fare worse still (Case et al., 2003). According to the authors, much of the gap between the schooling of orphans and non-orphans is explained by the greater likelihood that orphans will live with more distant relatives or unrelated caregivers Case et al., (2003). These findings, therefore, suggest the need for targeted interventions for orphans in the study area.
Table 3. Cross tabulation of selected (statistically significant) care provider socio-cultural factors against orphan care challenges.
| Care provider socio-cultural factors | Responses within background factors | |||
| Yes | No | |||
| Number | Percentage | Number | Percentage | |
| Relation to care provider *Clothing | ||||
| Paternal grandfather | 9 | 60 | 6 | 40 |
| Paternal grandmother | 18 | 36 | 32 | 64 |
| Maternal grandfather | 11 | 73.3 | 4 | 26.7 |
| Maternal grandmother | 28 | 62.2 | 17 | 37.8 |
| Paternal uncle/aunt | 53 | 61.6 | 33 | 38.4 |
| Maternal uncle/aunt | 56 | 72.7 | 21 | 27.2 |
| Other relatives/non-relatives | 83 | 62.9 | 49 | 37.1 |
| Chi-Square = 18.835 | ||||
| degrees of freedom = 6 | ||||
| p value (significant value) = 0.004** | ||||
| Relation to care provider *Parental love | ||||
| Paternal grandfather | 7 | 46.7 | 8 | 53.3 |
| Paternal grandmother | 18 | 36 | 32 | 64 |
| Maternal grandfather | 6 | 40 | 9 | 60 |
| Maternal grandmother | 25 | 55.6 | 20 | 44.4 |
| Paternal uncle/aunt | 51 | 59.3 | 35 | 40.7 |
| Maternal uncle/aunt | 50 | 64.9 | 27 | 35.1 |
| Other relatives/non-relatives | 80 | 60.6 | 52 | 39.1 |
| Chi-Square = 14.221 | ||||
| degrees of freedom = 6 | ||||
| p value (significant value) = 0.027** | ||||
| Relation to care provider *education | ||||
| Paternal grandfather | 8 | 53.3 | 7 | 46.7 |
| Paternal grandmother | 25 | 50 | 25 | 50 |
| Maternal grandfather | 9 | 60 | 6 | 40 |
| Maternal grandmother | 36 | 80 | 9 | 20 |
| Paternal uncle/aunt | 64 | 74.4 | 22 | 25.6 |
| Maternal uncle/aunt | 63 | 81.9 | 14 | 18.2 |
| Other relatives/non-relatives | 99 | 75 | 33 | 25 |
| Chi-Square = 21.770 | ||||
| degrees of freedom = 6 | ||||
| p value (significant value) = 0.001** | ||||
Source: Researchers, 2015
In a rural Zimbabwean study, an attempt to describe how AIDS has impacted on extended family orphan care arrangements, Nyamukapa and Gregson used a combination of both qualitative and quantitative data to explain the initial absence, followed by emergence of differentials in primary school enrolment between orphans and non-orphans in rural Zimbabwe. The duo found that maternal but not paternal or double orphans have lower primary school completion rates than non-orphans, and that these patterns reflect adaptations and gaps in extended family orphan care arrangements (Nyamukapa et al., 2005).
Current marital status of a care giver was found to be significantly related to orphan access to food (X2 = 11.568; df = 3 and p < 0.05), and show of parental love (X2 = 7.926; df = 3 and p < 0.05) (see Table 2). Orphans living with care providers who had never married and those currently in marital unions, compared to other marital status categories were more likely to report having experienced lack of food and/or parental love. Widowed and divorced care providers are often documented to be more disadvantaged than those care providers in marriage in terms of access to material means of care. However, they are more likely to be understanding of orphans since some of them also have their own orphans. Orphans under the care of married couples are likely to experience competition for care resources from those of care providers, often a source of conflict. It is also documented that orphans living with young care providers including child headed households are likely to face challenges related to access to basic needs including education. The following statements from orphan discussants captured the overwhelming and frustrating nature of orphan care especially among the very young and elderly care providers without means of proper care.
They (care providers) do not have enough money to provide for us, especially food, school fees and paraffin for study. They are often in dilemma to choose what to buy between food and paraffin (A boy of 17 years, Form 2, Kombewa Division).
I agree with the rest (other discussants), most care providers go for otong’o (weeding for others for pay) for them to put food on the table. Some of us go many times without super at night (A girl of15 years, class 7, Kombewa Division).
Such frustration is an indication that the extended family is overwhelmed with orphan care (Foster et al., 1995). Urassa and others argued that the prevalence of paternal uncles and aunts in taking care has gone down leaving care in the hands of more and more widowed grandparents, maternal relatives and siblings (Urassa et al., 2003). In the case of those care providers who reportedly had never been married (who are likely to be young), Robinson and others, in a study in three countries of Lesotho, Tanzania and Zimbabwe argued that the range of caring tasks that young people engage in have tremendous impact on their physical and emotional well-being, education and income (Robinson et al., 2006). Such stresses were likely to have negative effect on those under their care as well.
3.11. Socio-Economic Factors
Current place of residence (rural or urban) of care provider was also found to be significantly linked to orphan access to food (X2 = 6.707; df = 1 and p < 0.05), and exposure to stigma (X2 = 3.960; df = 1 and p < 0.05) (see Table 4). Orphans living with care providers in urban areas were more likely to report having experienced lack of food and exposure to stigma than their rural counterparts. Though not related to specific place of residence, a study in Kenya by Juma and others found that orphans reported less supervision by adults at home, and perceived that they were less loved at home than non-orphans (Juma et al., 2007). This is plausibly expected to worsen in urban areas due to individualistic lifestyle (Ocholla-Ayayo, 1997).
Table 4. Cross tabulation of selected (statistically significant) care provider socio-economic factors against orphan care challenges.
| Care provider socio-economic factors | Responses within background factors. | |||
| Yes | No | |||
| Number | Percentage | Number | Percentage | |
| Place of residence *Food | ||||
| Urban | 203 | 71.2 | 82 | 28.8 |
| Rural | 79 | 58.4 | 56 | 41.6 |
| Chi-Square = 6.707 | ||||
| degrees of freedom = 1 | ||||
| p value (significant value) = 0.010* | ||||
| Place of residence *Stigma | ||||
| Urban | 181 | 63.5 | 104 | 36.5 |
| Rural | 72 | 53.3 | 63 | 46.7 |
| Chi-Square = 3.960 | ||||
| degrees of freedom = 1 | ||||
| p value (significant value) = 0.047* | ||||
| Highest level of education *Food | ||||
| No formal education | 52 | 56.5 | 40 | 43.5 |
| Primary education | 108 | 66.3 | 55 | 33.5 |
| Secondary education | 73 | 70.2 | 31 | 29.8 |
| Tertiary education | 24 | 77.4 | 7 | 22.8 |
| University education | 25 | 83.3 | 5 | 16.7 |
| Chi-Square = 10.249 | ||||
| degrees of freedom = 4 | ||||
| p value (significant value) = 0.036* | ||||
| Highest level of education *Stigma | ||||
| No formal education | 43 | 46.7 | 49 | 53.3 |
| Primary education | 102 | 62.6 | 61 | 37.4 |
| Secondary education | 67 | 64.4 | 37 | 35.6 |
| Tertiary education | 23 | 74.2 | 8 | 25.8 |
| University education | 18 | 60.0 | 12 | 40.0 |
| Chi-Square = 10.653 | ||||
| degrees of freedom = 4 | ||||
| p value (significant value) = 0.031* | ||||
Source: Researchers, 2015
Table 5. Cross tabulation of selected (statistically significant) care provider socio-economic factors against orphan care challenges.
| Care provider socio-economic factors | Responses within background factors | |||
| Yes | No | |||
| Number | Percentage | Number | Percentage | |
| Highest level of education *Parental love | ||||
| No formal education | 43 | 46.7 | 49 | 53.3 |
| Primary education | 101 | 62.0 | 62 | 38.0 |
| Secondary education | 52 | 50.0 | 52 | 50.0 |
| Tertiary education | 22 | 29.0 | 9 | 29.0 |
| University education | 19 | 36.7 | 11 | 36.7 |
| Chi-Square = 10.539 | ||||
| degrees of freedom = 4 | ||||
| p value (significant value) = 0.032* | ||||
| Type of employment*Food | ||||
| Unemployed/unengaged | 72 | 66.1 | 37 | 33.9 |
| Formally employed | 51 | 86.4 | 8 | 13.6 |
| Informally employed | 159 | 63.1 | 93 | 36.9 |
| Chi-Square = 11.889 | ||||
| degrees of freedom = 2 | ||||
| p value (significant value) = 0.003** | ||||
| Type of employment*Sexual abuse | ||||
| Unemployed/unengaged | 42 | 38.5 | 67 | 61.5 |
| Formally employed | 26 | 44.1 | 35 | 55.9 |
| Informally employed | 67 | 26.6 | 185 | 73.4 |
| Chi-Square = 9.453 | ||||
| degrees of freedom = 2 | ||||
| p value (significant value) = 0.009* | ||||
| Type of employment*Physical abuse | ||||
| Unemployed/unengaged | 55 | 50.5 | 54 | 49.5 |
| Formally employed | 41 | 69.5 | 18 | 30.5 |
| Informally employed | 124 | 49.2 | 128 | 50.8 |
| Chi-Square = 8.105 | ||||
| degrees of freedom = 2 | ||||
| p value (significant value) = 0.017** | ||||
| Type of employment*education | ||||
| Unemployed/unengaged | 75 | 68.8 | 34 | 31.2 |
| Formally employed | 51 | 86.4 | 8 | 13.6 |
| Informally employed | 178 | 70.6 | 74 | 29.4 |
| Chi-Square = 6.915 | ||||
| degrees of freedom = 2 | ||||
| p value (significant value) = 0.032** | ||||
Source: Researchers, 2015
Additionally, care provider level of education was found to be significantly related to orphan access to food (X2 = 10.249; df = 4 and p < 0.05); show of parental love (X2 = 10.539; df = 4 and p < 0.05), and stigma experience (X2 = 10.653; df = 4 and p < 0.05) (see Table 4). Also, care provider employment status was found to be significantly related to orphan access to food (X2 = 11.889; df = 2 and p < 0.05); education (X2 = 6.915; df = 2 and p < 0.05); exposure to sexual abuse (X2 = 9.453; df = 2 and p < 0.05), and physical abuse (X2 = 8.105; df = 2 and p < 0.05). Orphans living with care providers of relatively higher levels of education (tertiary and university), and who were in formal employment were more likely to report lack of food and parental love, and to be exposed to stigma, and physical and sexual abuse. Care provider level of education and employment status could be linked to his/her place of residence (mostly urban).
Most care providers who are relatively highly educated and formally employed were likely to be found in urban centres, hence similar effects on orphan access materials, services and rights as discussed elsewhere in this study. For instance, urban centres have variously been documented as areas of individualistic life with weak social networks and support systems (Ochola-Ayayo, 1997). This was conceivably likely to promote stigma, abuse and a feeling of lack of parental love among orphans. Strict feeding arrangement coupled with smaller food rations due to high cost of living in urban areas could perhaps explain reportedly less access to food among orphans in the urban areas. Additionally, other children in the household may see orphans as strangers or intruders hence high reported cases of orphan abuse. In this study, a number of orphans were reportedly physically and sexually abused by the elder children of their care providers, particularly in the city.
The following statements by affected orphans living in some of the up-market areas of urban Winam Division help explain what many orphans go through.
Most orphans are sexually abused, especially girls. Care provider’s male adult children usually do this. It happened to me and when I reported the case, the family accused me of creating stories to win their favor (A girl of16 years, Form 3, Winam Division).
While others may love you, some of the relatives may hate you so much without any reason. Like where I am staying, one of the elder daughters (to my aunt) just hates me. She one day slapped me badly until I fell without any reason. She is like a chameleon, sometimes she is good but sometimes she is bad (A boy of 14 years, Class 7, Winam Division).
On the contrary, a survey carried out by Population Council in Nyanza reported that non-orphans were more likely to report having been beaten in the previous 12 months compared to orphans. Guardians might have felt uneasy disciplining orphans who are not their own children fearing that the children may interpret this as abusive rather than as a form of guiding the child (Population Council, 2007). Other care provider background factors though important and related to the orphan care needs, were found to be statistically insignificant.
3.12. Orphan Care Challenges and Orphan Migration
Table 6. Logistic regression results of orphan care need factors and orphan migration.
| Challenge | (ß) | SE | Wald | df | Sig. | Exp (ß) |
| Food | -4.036 | 0.657 | 37.763 | 1 | 0.000*** | 0.018 |
| Stigma | -1.327 | 0.465 | 8.144 | 1 | 0.004** | 0.265 |
| Shelter | -0.529 | 0.401 | 1.735 | 1 | 0.188 ns | 0.589 |
| Clothing | 0.058 | 0.453 | 0.016 | 1 | 0.898 ns | 1.060 |
| Sexual abuse | -0.431 | 0.491 | 0.771 | 1 | 0.380 ns | 0.650 |
| Health care | 0.540 | 0.544 | 0.985 | 1 | 0.321 ns | 1.716 |
| Physical abuse | -1.425 | 0.643 | 4.918 | 1 | 0.027* | 4.160 |
| Parental love | -0.476 | 0.595 | 0.641 | 1 | 0.427 ns | 0.621 |
| Education | -1.817 | 0.467 | 15.133 | 1 | 0.000*** | 0.162 |
| Play | -0.873 | 0.602 | 2.105 | 1 | 0.147 ns | 0.418 |
| Inheritance | -0.385 | 0.472 | 0.666 | 1 | 0.414ns | 0.680 |
| Other | 0.611 | 0.786 | 0.605 | 1 | 0.437 ns | 1.843 |
| Constant | 3.076 | 0.488 | 39.690 | 1 | 0.000*** | 21.676 |
| Note: The model -2Log Likelihood = 189.038; Model Chi-square = 320.654 at p<0.001; overall percentage = 91.4 percent; number of cases = 420; Nagelkerke R-square = 0.760; ß = Regression coefficient; SE = Standard error of the estimate; Wald = Wald statistics depicting relationship between dependent and independent /intermediate variables; df = degree of freedom; Exp(ß) = odds ratio or probability of event occurring over probability of event not occurring; Sig. = significance level or p values; *, **, *** statistically significant at p<0.05, 0.01 and 0.001 levels respectively; and ns = not significant at 0.05, 0.01 and 0.001 level of significance. | ||||||
Source: Researchers, 2015
Overly, the Wald logistic regression model fitted well to the data as evident in significance level value (p < 0.05) of the constant. The - 2 Log likelihood of 189.038 implies overall good fitness of data to the model, whereas the overall percentage of 91.4 percent signifies correct predictions of the intermediate variables by the model. The model Chi-square of 320.654 at p < 0.05 and df = 12 implies significant influence of these selected independent intermediate variables on the dependent variable. Nagelkerke R2of 0.760 shows a strong positive correlation between the selected independent variables and the dependent variable (see Table 5).
Access to food and education, and exposure to stigma and physical abuse were found to be significantly related to orphan migration. It could, therefore, be argued that although these four intermediate independent factors were statistically significant in triggering orphan migration, the contribution of the other factors was equally important, though not statistically significant at p < 0.05 (see Table 5). The following statements from affected orphans better espouse the survival nature of most orphans and their linkage to orphan migration.
Orphan movement depends on how you are treated. If one treats you badly, you move to another relative. Movement of orphans is just a cycle (A boy of 17 years, Form 3, Winam Division).
When the time for eating comes, orphans are given small portions compared to the children of the home, or sent to go and draw water or do any other work and by the time s/he comes back, all other people shall have finished eating and s/he is given fragments. And in case they ask for money, the children of the home are given while the orphan is told that there is no money, they should look for it elsewhere (A boy of 16 years, Class 6, Kombewa Division).
In Kenya, migration has been observed among orphans who wish to look for waged employment especially when they realize that they do not have further opportunity for schooling, and when working is presented as the only feasible alternative (Nyambedha et al., 2003). This has been confirmed in similar studies (Ansell et al., 2004; Guest, 2003; Barnett et al., 2002, and Ledward, 1997).
The greatest challenge most orphan foster care providers faced across the board, according to the opinion leader and orphan discussants and interviewees, was lack of means to cater for their basics of life including education. This was cited also by a majority of foster care providers who felt rather frustrated that they were unable to meet all the basic needs of the orphans under their care. They reportedly lacked meaningful income and the needed financial and/or material support to meet the basic needs of their own families let alone the orphan. Depletion of one’s own and family resources because of overwhelming AIDS-related medical care needs for sick relatives, their funeral expenses when they die, and orphan care needs have been cited as big challenges (Young, 2004; Nyambedha et al., 2003; UNICEF, 2003). A good number had to suspend personal or family plans to care for and support the orphans. A few foster care providers felt disappointed with the fact that some orphans under their care were never satisfied with care and support efforts however hard they (care providers) tried.
Surprisingly, some care providers reportedly had not been affected at all by orphan care. This could perhaps be due to genuine self sufficiency in meeting orphan care needs or an indication of an emerging "don’t care attitude" among some caregivers as mentioned by a number of orphans during FGDs. A number of foster care providers, however, recognized orphan care as a humbling experience with a lot to learn from. The following statements captured the overwhelming and frustrating nature of orphan care both within the rural and urban communities.
They (care providers) do not have enough money to provide for us, especially food, school fees and paraffin for study. They are often in dilemma to choose what to buy between food and paraffin (A boy of 17 years, Form 2, Kombewa Division)
There is no money (to buy food) to feed us and sometimes my aunt and my uncle shout at each other. We end up sleeping without supper (A girl of 14 years, class 6, Winam Division.)
I agree with the rest (other discussants), most care providers go for otong’o (weeding for others for pay) for them to put food on the table. Some of us go many times without super at night (A girl of15 years, class 7, Kombewa Division).
Jaber’s (not real name) father was my best friend. He died in 2007 when Jaber was 12 years old. A few months before he died, he had asked me not to let his children suffer especially Jaber. Therefore, when he finally died, I took Jaber to my home and she is now in form 3. I have two wives and six children to look after as well. It is really a burden but God is there… (A 58 year old foster care provider, Kombewa Division).
In addition, communication between orphans and their care providers was reportedly limited. Most care providers did not share their challenges with the orphans. In fact, some were reported to have no time for the orphans under their care. This existed despite the fact that some orphans contributed substantially to the host family financially. Lack of communication was cited by the discussants to often lead to misunderstanding hence strained relationship between orphans, particularly older ones and their care providers. The orphans would be very happy to share in the frustrations and challenges of their care providers as depicted in the following statements.
My care provider does not share with me. She does not talk to me. She does not feel like talking to me. I eat when I get and I do not complain. We orphans would really wish our care providers shared with us the challenges they go through (to care for us). This will help us understand the situation better and the reason why there is no food (A boy of17 years, class 7, Kombewa Division).
We orphans will sometimes realize that there is no food in the house when the care provider becomes so cruel to us (A girl of 15 years, class 7, Kombewa Division).
No (she does not share). However, I really like the issue of my stepmother sharing the challenges with me because I will get to realize that the little that there is has to be used economically. I will avoid wasting things because we are not going to get any other soon (A girl of16 years, Form 3, Winam Division).
4. Conclusions and Recommendations
4.1. Conclusions
4.1.1. Orphan characteristics and Orphan Care Challenge
It was established that some orphan care challenges could be attributable to an orphan’s own background characteristics. Orphan background characteristics including sex and level of education (age) was significantly linked to specific orphan care needs including access to food, shelter, clothing and school attendance, and exposure to stigma. Sex of an orphan was significantly associated with exposure to stigma, access to food and school attendance, cases of which the female gender orphan was mostly disadvantaged. Again, despite the fact that lack of shelter and clothing affects orphans of almost all ages, older ones in secondary schools were understandably more likely to report lacking such basics compared to their younger counterparts, perhaps, because of differences in their developmental needs with age.
4.1.2. Care Provider Characteristics and Orphan Care Challenge
It has been demonstrated that care provider background characteristics including sex, place of residence, current marital status, employment status, level of education, and relation to orphan were significantly associated with orphan access to food and clothing, and exposure to stigma, and physical and sexual abuse. Orphans, particularly girls, living with female care providers were more likely to experience sexual abuse than those living with male care providers. Current place of residence (rural or urban) of care provider was also found to be significantly linked to orphan access to food and exposure to stigma. Orphans living with care providers in urban areas were more likely to report having experienced lack of food and exposure to stigma than their rural counterparts. Current marital status of a care giver was found to be significantly related to orphan access to food, and show of parental love. Orphans living with care providers who had never married and those currently in marital unions, compared to other marital status categories were more likely to report having experienced lack of food and/or parental love. Care provider level of education was found to be significantly related to orphan access to food, show of parental love, and stigma experience.
Also, care provider employment status was found to be significantly related to orphan access to food, education, exposure to sexual and physical abuse. Orphans living with care providers of relatively higher levels of education (tertiary and university), and who were in formal employment were more likely to report lack of food and parental love, and to be exposed to stigma, and physical and sexual abuse. Care provider level of education and employment status could also be linked to his/her place of residence (mostly urban) as discussed elsewhere. Care provider relation to the orphan was significantly related to access to food, clothing, education and show of parental love by the orphan. In most cases, living with uncle/aunt from either paternal or maternal side of the family was found to be disadvantageous to an orphan with regard to access to most basic care needs.
4.1.3. Orphan Care Challenges and Orphan Migration
Access to orphan care needs like food and education and exposure to stigma and physical abuse were found to significantly likely to trigger orphan migration. Indeed depletion of one’s own and family resources because of overwhelming AIDS-related medical care needs for sick relatives, their funeral expenses when they die, and orphan care needs were the main factors linked to inability of most affected households to properly care for orphans under their care.
4.2. Recommendations
4.2.1. Research Recommendations
Isolating HIV and AIDS related orphanhood remained a major challenge to this study. This was partly because obtaining hospital data linking parental deaths in Kenya, like in most third world countries was not possible. This was due to ethical and confidentiality concerns and the complicated nature of opportunistic infections related to an AIDS patient at the point of death. This study recommends the use of other cause specific methods to more precisely capture the magnitude of orphanhood that could be attributable to HIV and AIDS epidemic per se.
The study revealed that while some orphans moved, others did not. It would be interesting to further investigate why, faced with almost similar care environments, some orphans would move while others would choose to stay.
4.2.2. Policy Recommendations
Orphan mobility was found to be a reality with back and forth movements in Kisumu District. This has altered the occurrence and distribution considerably in the study area. The study recommends that in the short run, the governmental and non-governmental agencies should offer material and technical support to existing orphan care institutional arrangements to better care for the orphans and hence curb high orphan mobility in the study area. On the long-term, high structural poverty levels in the region needs to be addressed to enable the community cope better in the management of orphans in order for them to participate fully in the future development of the country.
Abbreviations
| AIDS | Acquired Immune Deficiency Syndrome |
| FGD | Focus Group Discussion |
| GoK | Government of Kenya |
| HIV | Human Immuno-deficiency Virus, the virus that causes AIDS. |
| IDI | In-Depth Interview |
| UNAIDS | United Nations Programme on HIV and AIDS |
| UNICEF | United Nations Children’s Fund |
| USAID | United States Agency for International Development |
| WB | World Bank |
References
- Ainsworth, M., and D. Filmer (2002): Poverty, AIDS and Children’s Schooling: A Targeting Dilemma. World Bank Policy Research Working Paper 2885. Washington, D.C: The World Bank.
- Ansell, N. and L. Young (2004): Enabling Households to Support Successful Migration of AIDS Orphans in Southern Africa. In: AIDS Care 16: 1, 3-10. Taylor and Francis, London.
- Atwine B., E. Cantor-Graae and F. Banjunirwe (2005): Psychological Distress among AIDS Orphans in Rural Uganda. In: Social Science & Medicine, (61): 555-564.
- Barnett, T., and A. Whiteside (2002): AIDS in the Twenty-First Century. Disease and Globalization. Palgrave Macmillan, New York.
- Bicego, G., S. Rutstein, and K. Johnson (2003): Dimensions of the emerging orphan crisis in sub-Saharan Africa. In: Social Science and Medicine. 56: 1235-1247.
- Case A., D. Paxson, J. Ableidinger (2003): The Education of African Orphans. Centre for Health and Well Being. Research Program in Development, Princeton University.
- Cattel, M. G. (1993): Caring for the Elderly in sub-Saharan Africa. Ageing International.
- Crampin, A. C., S. Floyd, J. R. Glynn, N. Madise, and Others (2003): The Long-term Impact of HIV and Orphan-hood on the Mortality and Physical Well-being of Children in Rural Malawi. In: AIDS 17(3): 389-397.
- Dawes, A., and M. Mushwana (2007): Monitoring Child Abuse and Neglect. In: Dawes, A., A. Bray, and A. Van der Merwe (eds): Monitoring Childrights and Wellbeing. A South Africa Approach. Cape Town, HSRC Press.
- Deininger, K., M. Garcia and K. Subbarao (2003): AIDS-Induced Orphanhood as a Systematic Shock: Magnitude, Impact, and Program Interventions in Africa. In: World Development Vol. 31, No. 7, pp. 1201-1220. Pergamon, Elsevier Science Ltd.
- Drew R.S., C. Makufa, and G. Foster (1998): Strategies for Providing Care and Support to Children Orphaned by AIDS. In: AIDS Care. Suppl. 1:S9-15.
- Ensminger, J. (1992): Making a Market. The Institutional Transformation of an African Society. Cambridge. Cambridge Press.
- Foster, G., C. Makufa, R. Drew, S. Mashumba and S. Kambeu (1997): Perceptions of Children and Community Members Concerning the Circumstances of Orphans in Rural Zimbabwe. In: AIDS Care. 9(4): 391-405.
- Foster, G., R. Shakespeare, F. Chinemana, H. Jackson, S. Gregson, C. Marange, and S. Mashumba (1995): Orphan prevalence and Extended Family Care in Peri-urban Community in Zimbabwe. In: AIDS Care. Vol. 7, Issue 1, 1995.
- Ghosh, J. and E. Kalipeni (2004): Rising Tides of Orphans in Southern Africa. Kalipeni, E. S. Craddock, J. R. Oppong and J. Ghosh (eds.): HIV and AIDS in Africa. Beyond Epidemiology, 304-16. Blackwell, Malden, Oxford, Carlton.
- G.o.K., (2010): 2009 Population and Housing Census. Nairobi. Government Press.
- Gregson, S., C. Nyamukapa, G. P. Garnett, M. Wamba, J. J. C. Lewis, P. R. Mason, S. K. Chandiwana, and R. M. Anderson (2005): HIV-infection and Reproductive Health in Teenage Women made Vulnerable by AIDS in Zimbabwe. In: AIDS Care. 17.7, 785-94.
- Guest, E. (2003): Children of AIDS: Africa’s Orphan Crisis. (2nd Edition). London: Pluto Press.
- Hosegood, V. and I. Timaeus (2003): Household Composition and Dynamics in KwaZulu Natal, South Africa: Mirroring Social Reality in Longitudinal Date Collection. In: African Household, Ed. Etienne van de Walle, University of Pennsylvania.
- Hosmer and Lameshow (1989): "Applied Logistic Regression" Wiley-inter Science Publication. John Wiley and Sons, New York.
- Howard B.H., C.V. Phillips, N. Matinhure, K.J. Goodman, S.A. McCurdy and C.A. Johnson (2006): Barriers and Incentives to Orphans Care in a Time of AIDS and Econimc Crisis: A Cross-sectional Survey of Caregivers in Rural Zimbabwe. In: BMC Public Health. (6):27.
- Jewkes, R., J. Lewis, and L. A. Penn-Kekana (2003): Gender Inequalities, Intimate Partner Violence and HIV Prevention Practices: Findings of a South African Cross-sectional Study. In: Social Science and Medicine. 56.1, 25-43.
- Joint United Nations Program on HIV and AIDS (UNAIDS) (2002): Report on the Global AIDS Epidemic. Geneva, UNAIDS.
- Juma, M., I. Askew, and A. Ferguson (2007): Situation Analysis of the Sexual and Reproductive Health and HIV Risks and Prevention Needs of Older orphaned and Vulnerable Children in Nyanza Province, Kenya. Nairobi, Department of Children Services, Government of Kenya.
- Ledward A. (1997): "Age, Gender and Sexual Coercion: Their Role in Creating Pathways of Vulnerability to HIV Infection". Masters Dissertation, M Sc Medical Anthropology. London: University of London.
- Lee, T. (2000): Evaluating Community-based Orphan Care in Zimbabwe (available athttp://www.hivnet.ch:800/topic/care/review?60.
- Lusk and Others (2003): Community Care for Orphans and AIDS Affected Children. In: Speak for the Child. Academy for Educational Development.
- Makame V., C. Ani, S. Grantham-McGregor (2002): Psychological Well-being of Orphans inDar El Salaam, Tanzania. In: Acta Paediatr Index Medicus. 2002; 91(4):459-465.
- Mawoneke, S., A. Sexton, and K. Moyo (2001): AIDS and Street Children in Zimbabwe.
- Miles, M. B., and A. Huberman (1998): Qualitative Data Analysis: A Sourcebook of New Methods. Newbury Park, CA: Sage Publications.
- Ministry of Planning, National Development and Vision 2030 (2009): Kisumu East District Development Plan 2008-2012. Nairobi, Government Press.
- Mishra, V. F. A., F. Otieno, A. Cross and R. Hong (2005): Education and Nutritional Status of Orphans and Children of HIV-infected Parents in Kenya. No. 24, ORC Macro, Demographic and Health Research Division, Calverton, Maryland.
- Monasch and J. Boerma (2004): Orphanhood and Childcare Patterns in sub-Saharan Africa: Analysis of National Surveys from 40 Countries. In: AIDS 18 (suppl. 2): S55-S65
- Mutangadura, G. B., (2001): Women and AIDS in Southern Africa: The case of Zimbabwe and its Policy Implications. In: Jenda: A journal of Culture and African Women studies 1(2): 1-11.
- Muula, A., H. Misiri, L. Munthali, S. Kalengo, F. Kacheli, M. Mbewe, and S. Msuku (2003): The Living Situation of Orphans in Peri-urban, Blantyre, Malawi. In: South Africal Medical Journal. 93.12, (920-1).
- Ntozi, J.P.M, (1997):Effect of AIDS on children: the problem of orphans in Uganda. In: Health Transition Review 7(supp.): 23-40.
- Nyambedha E. O., S. Wandiba and J. Aagaard-Hansen (2003): Changing Patterns of Orphan Care due to HIV Epidemic in Western Kenya. In: Social Science and Medicine (57): 301-311.
- Nyamukapa C. A., Foster G., Gregson S. (2003): Orphans’ Household Circumstances and Access to Education in a Maturing HIV-epidemic in Eastern Zimbabwe. In: Journal of Social Development in Africa. 18(2): 7-32.
- Nyamukapa, C. and S. Gregson (2005): Extended Family’s and Women’s Roles in Safeguarding Orphans’ Education in AIDS-affected Rural Zimbabwe. In: Social Science Medicine. 60(10): 2166-67.
- Ocholla-Ayayo, A.B.C. (1997): HIV-Risk Factors and Changing Sexual Practices in Kenya. In: Africa Families and the Crisis of Social Change, Westport
- Oleke, C., A. Blystad, K. Fylkesnas, and J. K. Tumwine (2007): Constraints to Educational Opportunities of Orphans: A Community Based Study from Northern Uganda. In: AIDS Care. 19.3, (361-8).
- Owiti E. A. (2004): The Care of Orphans and Vulnerable Children in Kenya: A Cost Effective Analysis. M.A. Thesis (unpublished), University of Nairobi. Nairobi.
- Population Council (2007): The Role of Schools in Promoting Sexual and Reproductive Health among Adolescent in Developing Countries. Population Council.
- Robinson, E., Ansell, and Others (2006): Young Caregivers in the Context of HIV/AIDS Pandemic in sub-Saharan Africa. In: Population, Space and Place, Vol. 12 (93-111).
- Salaam T. (2005): AIDS Orphans and Vulnerable Children (OVC): Problems, Responses and Issues for Congress. Congressional Research Service.
- Silverman, D. (2006): Interpreting Qualitative Data: Methods for Analyzing Talk, Text and Interaction. 3rd Edition. London, Sage Publications.
- Subbarao K. and D. Coury (2004): Reaching out to Africa’s Orphans: A Framework for Public Action, The World Bank.
- The World Bank Group (2002): Education and HIV/AIDS, A Window of Hope. Washington DC. The World Bank.
- Thurman, T., L. Brown, L. Richer, P. Maharaj, and R. Magnani (2006): Sexual Risk Behaviour among South African Adolescents: Is Orphan Status a Factor? In: AIDS and Behaviour. 10.6, (627-35).
- UNAIDS (2008): 2010 UNAIDS Report on the Global AIDS Epidemic.
- UNICEF (2010): Kenya Statistical Data Sheet. (available at http://www.unicef.org/infoby country/kenya_statistics.htm). (retrieved in May 2011).
- UNICEF, UNAID Sand USAID (2002): Children on the Brink 2002: A joint report on orphan estimates and program strategies. Washington, DC: UNAIDS, UNICEF, and USAID.
- United Nations Children’s Fund (1998): Community Based Orphan Assistance in Malawi: Demographic Crisis as Development Opportunity, UNICEF.
- United Nations Children’s Fund (1999): Children Orphaned by AIDS; Frontline Responses from Eastern and Southern Africa. UNICEF.
- United Nations Children’s Fund (2003): Africa’s Orphaned Generation. In: Africa’s Orphans. UNICEF.
- United Nations Children’s Fund (2006): Africa’s Orphaned and Vulnerable Generation: Children Affected by AIDS, UNICEF.
- United States Agency for International Development, SCOPE-OVC and Family Health International (2002): Results of the Orphans and Vulnerable Children Head of Household Baseline Survey in Four Districts in Zambia.
- Urassa, M. J. T. Boerma, R. Isingo and others (2001): The Impact of HIV/AIDS on Mortality and Household Mobility in Rural Tanzania. In: AIDS 15 (15): 2017-2023.
- Urassa, M., T. Boerma, Z. Ng’eweshemi, R. Isingo, D. Schapink, and Y. Kumogola (2003): Orphanhood, Child Fostering and the AIDS Epidemic in Rural Tanzania. In: Health Transition Review 7 (Suppl. 2), 1-5.
- Utan, K. (2005): Collateral Damage: HIV/AIDS Creates a Generation of Orphans and Vulnerable Children. In: Common Health. Spring 2005
- Wuensch, K. L. (2004): Logistic regression with SPSS. (available athttp://core.ecu.edu/psyc/wuenschk/SPSS/SPSS-Data.htm), retrieved on 18/02/2010.
- Yamano, T., and T. S. Jayne (2004): Measuring the Impact of Working-age Adult Mortality on Small-scale Farm Households in Kenya. In: World Development 32(1): 91-119.
- Young L. (2004): Journeys to the Street: The Complex Migration Geographies of Uganda Street Children. In: Geoforum 35(4): 471-488.



