Public Health and Preventive Medicine, Vol. 1, No. 3, August 2015 Publish Date: Jun. 24, 2015 Pages: 101-107
Impact of Choir Singing in Elderly on Depression Symptoms and Voice Quality
Mauriceia Cassol1, Angelo Jose Goncalves Bos2, *
1Department of Speech and Audiology, Federal University of Health Sciences of Porto Alegre, Porto Alegre, Brazil
2Graduate Program on Biomedical Gerontology, Institute of Geriatrics and Gerontology, Pontifical Catholic University of Rio Grande do Sul, Porto Alegre, Brazil
Abstract
Purpose: The purpose of this study is to verify possible changes in depression and vocal quality in older-adults who engaged in a two-year choir singing activity. Methods: This study has a longitudinal and experimental design. The study group consisted of older-adults, 8 males and 36 females, ranging from 60 to 80 years of age, with an average of 67 years. Depression symptoms and voice quality were measured on each of the four evaluations: at the beginning of their participation in a choir singing activity (baseline) and three other evaluations: after 8 months, after 3 months (intermission), and 21 months. Depressive symptoms were questioned using the Yesavage Geriatric Depression Scale (GDS) and Vocal Quality (VQ) was measured using the GRBAS scale, two-way Analysis of Variance tested the statistical significance of the differences in GDS and VQ averages among the four evaluations. Pearson correlation coefficients assessed the association between changes in depression and changes in voice quality scores. Results: The mean GDS scores were 2.57, 1.30, 1.05, and 1.48, and the mean VQ were 2.18, 1.61, 1.59, and 1.11, respectively at baseline, after 8 months, after 3 months of intermission, and after 21 months. Depressive symptom reduction was significantly correlated to decrease in hoarseness but not to improvement in total vocal quality. Conclusions: Choir singing improves depressive symptoms and may play an important role in the treatment of emotional problems in the elderly, regardless of the vocal quality improvement. Choir participation should be encouraged to depressive elderly patients.
Keywords
Aging, Choir Singing, Voice Quality, Depression, Geriatrics
Received: April 9, 2015
Accepted:May 14, 2015
Published online: June 23, 2015
@ 2015 The Authors. Published by American Institute of Science. This Open Access article is under the CC BY-NC license. http://creativecommons.org/licenses/by-nc/4.0/
1. Introduction
Presbyphonia, or age-related dysphonia, can have a significant effect on the quality of life of the patient. The diminished ability to communicate might lead to loss of confidence, loss credibility, and social exclusion (1). In addition to the molecular effects of aging on the laryngeal tissues, the etiology of presbyphonia is often multifactorial because of comorbidities in the other organ systems involved in phonation. After a comprehensive evaluation, presbyphonia may be treated conservatively with voice therapy or with a range of interventions (2). Voice characteristics are not age specific and, under several aspects, are similar to those observed in some diseases and also in the frames of long vocal rest (3). The muscle disuse results in loss of muscle fibers so like to that observed in old age. If phonatory functions can be rehabilitated after vocal diseases and long periods of disuse, and if the changes observed are similar to the senescence, we should invest in the rehabilitation of oral communication of the elderly.
Emotional disturbances constitute a part in the array of oral communication disorders, and it can involve voice, articulation, speech sounds, fluency and language itself. Mental deviations may have clear vocal consequences (4). Among the most frequent emotional symptoms, depression is the one that strikes more often, being the most common psychiatric disorder among the elderly. Depressive symptoms are prevalent in elderly subjects, with a high societal cost (5). In a recent worldwide survey the World Health Organization identify the prevalence of Depression in 47 different countries finding that Depression had the lowest frequency in Africa (10%) and the highest in Europe (15%) concluding that it is a big public health problem (6).
Depression is associated with social isolation, higher mortality, and lower quality of life and self-esteem, mainly in the elderly (7, 8, 9). In addition, elderly patients tend to have higher prevalence of chronic degenerative diseases related to depressive symptoms. 10 Depressive symptoms improvements correlate with improvements in quality of life in the elderly (12). Depression is associated with obesity, higher prevalence of hypertension, osteoarthritis, urinary incontinence, and Parkinson disease (12, 13).
It is known that singing has beneficial effects on emotional status, resulting in well-being and improvement in depressive symptoms (14). Choir singing has also positive effects on immunologic and stress markers (15). Significant positive effect of voice training on vocal capabilities, mostly singing voice, is shown in several studies described.
The purpose of this study is to verify change of depression symptoms and improves vocal quality in elderly during a two-year choir singing activity.
2. Methods
2.1. Subjects
This study was longitudinal and experimental. The study was conducted during two years at the Pontifical Catholic University of Rio Grande do Sul (PUCRS), Brazil. A protocol was applied to check the profile of the studied population, as well as vocal health habits. The group study consisted of 44 older-adults individuals, 8 male and 36 female, ranging from 60 to 80 years of age, with an average of 67 years, who signed to participate in the Choral Singing Community Program "It is never late to sing". The participants had diverse occupations throughout their professional lives, having worked as teachers, businesspersons, salespersons, civil servants, secretaries, nurses and orderlies, homemakers, lawyers, and they had never been part of a choir group. During the selection of participants, no candidate displayed any neurological diseases, previous brain or neck surgery and history of depression. No participants referred the use of drugs for depression. During the study there was no indication pharmacological treatment. The project comprised 2-hour weekly choir rehearsals. The meetings, organized by an experienced conductor, consisted of relaxing exercises, posture guidelines, vocal technique, social reintegration, and self-esteem and motivation training.
2.2. Experimental Design
The beginning of this study coincided with the beginning of the choir activities at the University. All members of the choir received the same vocal training. After getting the explanation about the objectives, methodology, and privacy regarding data during the study, the participants who agreed to take part signed an informed consent term. The Ethics Committee (Internal Review Board) of PUCRS approved this study. The exclusion criteria were participants with presence of previous neurological and psychiatric diseases, such as Parkinson’s disease or previous stroke or had a history of brain or neck surgery. The total follow-up time was 21 months with a three-month intermission. There were four evaluations: the first took place before the beginning of the choir activity; the second 8 months later; the third 3 months afterwards; and the fourth after 21 months.
2.3. Assessment Techniques
Depression symptoms and voice quality were measured on each of the four evaluations. Depression symptoms were measured using Yesavage Geriatric Depression Scale (GDS), which consists of 15 questions with simple answers (yes/no). Each depressive answer is graded 1 point. Using this scale, individuals with 10 or more depressive answers are severely depressed, while between 5 and 10 they are mildly depressed, or bearers of a mild depression (16).
The perceptual-auditory vocal quality analysis was performed a silent environment requesting the vowel / a / sustained, and were recorded using a Sony digital voice recorder and a microphone Shure. A group of five voice specialists blinded to the sample evaluated the auditory data. The voice specialists received a form with items for evaluation and the voice recordings randomly assigned. The evaluations assessed (Figure 1), was used GRBAS scale (17), international considered as the gold standard in voice quality assessing (18, 19). This scale are evaluated changes in voice (Roughness, breathiness, asthenia, strain) and attributed a score of 0 to 3, considered zero degree without voice disorders, 1 mild, 2 moderate, and three severe dysphonia.
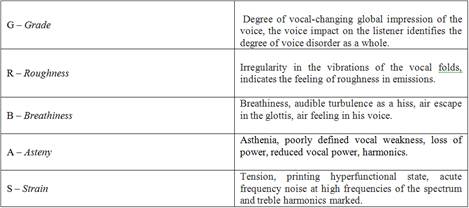
Figure 1. GRBAS Scale (Hirano, 1981).
2.4. Statistical Analysis
A two-way Analysis of Variance (ANOVA) tested the statistical significance of the differences in GDS and VQS averages of the four evaluations. When the comparison of the groups resulted in a significant ANOVA (p<0.05), the results of the second, third and fourth evaluations were compared with the first evaluation results using the Student’s t test for paired samples. Likewise, a value of p<0.05 was considered significant.
As noted above, VQS used the presence and severity of roughness, hoarseness, and breathiness. Correlation rates tested the statistical significance of the association between changes in depression level and changes in total VQS and in each vocal factor. Specifically, Pearson correlation assessed the association between improvement in depression and each of the following: improvement in total VQS, improvement in hoarseness, roughness and breathiness. Comparing individual differences of the assessments between the beginning of the program and eight weeks afterwards, between 8 and 12 weeks from the beginning and between 12 and 21 weeks, positive improvement got a code 1 (positive) negative changes received a -1 and no changes got a 0.
Following the statistical analysis, we performed a qualitative analysis of the behaviour changes observed through the answers given to depression questions in order to understand the possible effect of choir singing over these symptoms. Chi-square for trend was used to calculate the significance of the association between positive answer to each of depression symptoms and the assessment, with further pair chi-squared test were performed to assess the possible differences between the first assessment with the other three evaluations (after 8 months, After intermission, and after 21 months) A Fischer Exact test was uses when an expected cell less than 5 was observed.
3. Results
Table 1 shows the initial GDS and VQS averages, as well information on the sex and age of the participants. Figure 2 shows the graphic representation of the mean GDS and VQS in each step of the evaluation. ANOVA was significant for GDS among the four assessments (p<0.001). The average GDS at initial evaluation was significantly higher in than each other evaluation when tested by paired Student’s t tests (p<0.05).
Table 1. Distribution of participants according to sex, age and initial mean of GDS and VQS.
| Total | Women | Men | P | |
| Participants | 44 | 36 | 8 | |
| Mean age in years (sd) | 67.0 (6.29) | 66.4 (6.26) | 70.3 (5.82) | 0.136 |
| GDS mean (sd) | 2.57 (3.216) | 2.89 (3.398) | 0.86 (0.899) | 0.062 |
| VQS mean (sd) | 2.18 (1.529) | 2.27 (1.575) | 1.71 (1.254) | 0.164 |
GDS: Geriatric Depression Scale, VQS: Vocal Quality Scale
Figure 2 also shows a gradual and significant (ANOVA p<0.01) improvement in VQS in connection with choir singing. Mean of VQS at first evaluation were significantly higher than the other evaluations, when tested by paired Student’s t tests (p<0.01). The paired Student’s t test for VQS was significant in the comparison between the second and the last (p<0.01), but not the third evaluation, which was significant higher than the last evaluation (p<0.001). Among vocal parameters only roughness was significantly correlated with depression (Pearson correlation = 0.29, p<0.05).
Changes in relation to the voice disorders degrees showed at initial assessment 12 people (27%) had voice adapted or without voice alterations, 21 people (48%) had voice disorder in mild degree, 10 people (23%) had voice disorder moderate degree and one person (2%) presented voice disorder in severe degree. In the final assessment at 21 months, 25 people (57%) without voice alterations and 19 people (43%) voice disorder mild degree. The result of the chi-square test was significant (p=0.0106).
Table 2 presents the percentage distribution of the affirmative answers to the depression questions in the GDS. The GDS has 15 questions on depressive symptoms were 5 of them a "No" answer denotes depressive symptom and 10 of then a "Yes" expresses depressive mood. In general, the higher frequency of the answers expressed non depressive mood. The Chi-square test for trend was significant in 8 of the questions. The initial assessment was the period with most frequent depressive symptoms present. In general the second assessment presented the highest improvement, with improvement in 13 of the questions. There is a smaller improvement between the assessments after 8 months and after the intermission, with improvement in 7 questions and worsening or remaining the same in 4 other questions. The question with highest frequency of depressive answer was the question 2 about "have you given up many of your activities and interests?" with 41% of positive answers. The frequencies after 8 months and the intermission second presented the higher difference with the initial, being significant association (p<0.05). In the initial evaluation, 86% of the elderly stated were satisfied with their lives. As the evaluations progressed, the rate gradually increased until the end of the study when all participants seemed to be satisfied with their lives. Chi-square for trend was significant, but only the comparison between the initial and the last assessment was significant at Fischer Exact Test (p=0.0260). We also observed an important decrease in the number of elders who felt their lives were empty, showing little variation later. The association between feeling life empty and the participation in the Choral period was significant (p=0.0051). All posterior assessments presented a frequency significantly lower than the initial. The complaint about often feeling bored, reported by 18% of the elders, displayed a decline during their choir practice, then an increase after the intermission followed by a decline after 21 months. The number of elders who were in good mood most of the time increased at the beginning of the activities and remained the same throughout the study, 24% of the elders was afraid something bad might happen to them, and in the final evaluation, only 19% experienced that fear. Questions that presented the most significant Chi-square for trends were "Do you feel full of energy:" and "Do you think most of people are better off than you are?", almost all participants answered in a non-depressive way at after the intermission and after 21 months.

Figure 2. Depressive Symptoms (GDS) and vocal quality in each stage of the study.
Table 2. Percent distribution of the affirmative answers to each item Geriatric Depression Scale in each stage of the study.
| Geriatric Depression Sale (%) | Initial | After 8 Months | After intermission | After 21 months | P* |
| YES | YES | YES | YES | ||
| 1. Are you satisfied with your life in general? | 86 | 98 | 98 | 100† | 0.0037 |
| 2. Have you given up many of your activities and interests? | 41 | 16† | 19† | 24 | 0.1205 |
| 3. Do you feel your life is empty? | 29 | 4† | 5† | 10† | 0.0051 |
| 4. Do you often feel bored? | 18 | 10 | 19 | 17 | 0.9257 |
| 5. Are you in good mood most of the time? | 82 | 96† | 93 | 95† | 0.0407 |
| 6. Are you afraid something bad may happen to you? | 24 | 22 | 10† | 19 | 0.1964 |
| 7. Do you feel happy most of the time? | 90 | 98 | 98 | 88 | 0.6770 |
| 8. Do you often feel helpless? | 24 | 12 | 10† | 14 | 0.1296 |
| 9. Do you prefer to stay home instead of going out and doing new things? | 35 | 10† | 12† | 12† | 0.0086 |
| 10. Do you think you have more memory problems than most people do? | 31 | 20 | 14† | 17 | 0.0455 |
| 11. Are you happy to be alive now? | 94 | 94 | 100 | 100 | 0.0262 |
| 12. Are you worthless of the way you are now? | 6 | 4 | 2 | 2 | 0.2286 |
| 13. Do you feel full of energy? | 78 | 96† | 95† | 98† | 0.0012 |
| 14. Do you feel that your situation is hopeless? | 6 | 6 | 2 | 7 | 0.8896 |
| 15. Do you think most people are better off than you are? | 14 | 8 | 0† | 0† | 0.0014 |
* Chi-square for trend. †p<0.05 (Chi-square or Fischer Exact test with initial assessment).
4. Discussion
Group singing is probably one of the best exercises of social gathering. Six dimensions of benefits are associated with singing: benefits for well-being and relaxation, benefits for breathing and posture, social benefits, spiritual benefits, emotional benefits, and benefits for heart and immune system (20, 21).
This study followed a group of 44 older-adults for a 2 year period from the initial of a Choral Singing activity until the very last participation. We observed a positive relationship between choir singing and the decrease of depressive symptoms improvement voice quality in elderly. The musical activity can, therefore, have beneficial effects on the treatment of emotional problems associated with affective relations and be responsible for behaviour changes. In regards to all depressive symptoms evaluated by the GDS, there was an important and significant initial improvement. After three months of intermission, some individuals passed to demonstrate depressive symptoms again, leading to a light and not significant relapse in comparison to the second evaluation. This fact may result from the absence of social contact during the intermission period which supports the cause effect hypotheses that Choral Singing can decrease depressive symptoms and improve vocal quality. Similar observation was mentioned in a recent qualitative study of Skingley et al (22), following a singing group of older adults, whose subjective wellbeing benefits tended to "tail off" after the end of the activity.
The feeling of being helpless decreased after the beginning of the choir singing activities. Other aspects observed were that the number of elders who talked about feeling empty decreased after they joined the choir, and that the elders began to have a greater joy of living. It is important to point out that, at the end of evaluations (after 3 months of intermission and 21 months), no elderly in this study reported the feeling that most people had lives better than theirs. To have self-esteem, it is fundamental to value positive feelings, be optimistic, and face obstacles in a good mood (21). The authors observed a significant improvement of voice. For the perceptual evaluation, significant differences in grade of dysphonia, breathiness, and strained vocal quality were found.
Scientific studies have proved that music stimulates fundamental areas of the brain, such as those responsible for memory, muscle control and language. Some recovery from memory problem usually follows the improvement in depressive conditions (23).
The participants of this study began to use voice more intensely after entering the choir, engaging in several different activities such as volunteering, theatre groups and lecturing. We could observe significant changes between baseline and the follow-up assessments on depressive symptoms. In the literature, there are reports on best vocal results in physically active individuals, it can be inferred that the exercises help minimize the effects of age on voice (24). In a recent study, Hara et al (25) observed that satisfaction with verbal communication was positively associated to health related quality of life
Limitations of the Study:
The current study has two important limitations. A small sample size was not related to a dropout rate, but to those who engaged in the Choral Singing activity at the beginning of the Program, which started with all 44 followed participants. No dropout was observed during the follow-up period. The participants presented higher socioeconomic level than most older-adult Brazilians, thus the results might not be generalized to the whole population. The absence of Control Group was of a peculiar circumstance out of the author’s hand. The Choral Sing Project was not a research project and most of the older-adults who were contacted for Control Group actually engaged in the Choral during the first year of the follow-up, after knowing about the existence of the Project. At the end of the first year the choral participation reached almost a hundred participants. This paper, however, has its main strength on the longer follow-up time. In a recent review on beneficial effects of music therapy (26) in older-adults, most reviewed papers presented sample sizes lower than 35 participants with a maximum follow-up length of time of 6 months. The initial benefits of the choral participation remained almost constant during the 2 years of follow-up with some worsening or not improvement (in the case of vocal quality) after the intermission, corroborating with a cause-effect hypotheses and compensate the absence of the Control Group.
5. Conclusion
The results of this study show that choir improves depressive symptoms and vocal quality in elderly. The study showed a gradual reduction of the symptoms initially detected during the choir singing activities. The elders began to enjoy their lives better, experiencing a decline in boredom, fears over the future, feelings of desertion and helplessness, embarrassment and inferiority. They said they felt more lively, full of energy and happy with their lives, and made their activities and interests a priority. The choral singing is an important exercise for voice quality in elderly and to recover the effects of changes in the vocal folds caused by the aging process as the loss of collagen and elastin on the layers of the vocal folds. Additional research is needed with a case-control study for confirm these hypotheses.
References
- Etter NM, Stemple JC, Howell DM. Defining the Lived Experience of Older Adults with Voice Disorders. Journal of Voice. 2013 Jan; 27(1):61–67.
- Johns M M, Arviso LC, Ramadan F. Challenges and opportunities in the management of the aging voice. Otolaryngol Head Neck Surg. 2011 Jul;145(1):1-6.
- Goy H, Fernandes DN., Pichora-Fuller MK, van Lieshout P. Normative Voice Data for Younger and Older Adults. Journal of Voice. 2013 Sep; 27 (5):545–555.
- Behlau M. Voice: The Book of the Specialist II. Rio de Janeiro: Revinter, 2008
- Ekmana M, Granströmb O, Omérovc S., Jacobb J., Landénd M.. The societal cost of depression: Evidence from 10,000 Swedish patients in psychiatric care. Journal of Affective Disorders. 2013 Sep; 150(3): 790–797
- Loerbroks A, Bosch JA, Mommersteeg PMC, Herr RM, Angerer P, Li J. The association of depression and angina pectoris across 47 countries: findings from the 2002 World Health Survey. Eur J Epidemiol. 2014; 29:507–515 Available in: http://dx.doi.org/10.1007/s10654-014-9926-z.
- Iliffe S, Kharicha K, Harari, D, Swift C, Gillmann G, Stuck AE. Heath risk appraisal in older people 2: the implications for clinicians and commissioners of isolation risk in older people. Br J Gen Pract. 2007; 57:277–82.
- Kawamura T, Shioiri T, Takahashi K, Ozdemir V, Someya T. Survival rate and causes of mortality in the elderly with depression: a 15-year prospective study of Japanese community sample, the Matsunoyama-Niigata suicide prevention project. J Investig Med. 2007; 55:106–14.
- Sobocki P, Ekmam M, Agren H, Krakau I, Runeson B, Martensson B, Jonsson B. Health-related quality of life measured with EQ-5D in patients treated for depression in primary care. Value Health. 2007; 10:153–60.
- Moussavi S, Chatterji S, Verdes E, Tandon A, Patel V, Ustun B. Depression, chronic diseases, and decrements in health: results from the World Health Surveys. Lancet. 2007; 370:851–8.
- Gulmann NC, Lolk A. Depression in old age. Ugeskr Laeger. 2007;169:1462–5.
- Moreira RO, Marca KF, Appolinario JC, Coutinho WF. Increased waist circumference is associated with an increased prevalence of mood disorders and depressives symptoms in obese women. Eat Weight Disord. 2007; 12: 35–40.
- Gale N, Enright S, Reagon C, Lewis I, van Deursen R. A pilot investigation of quality of life and lung function following choral singing in cancer survivors and their careers. Ecancermedicalscience. 2012;6:261.
- Kreutz G, Bongard S, Rohrmann S, Hodapp V, Grebe D. Effects of choir singing or listening on secretory immunoglobulin A, cortisol, and emotional state. J Behav Med. 2004; 27:623–35.
- Siupsinskiene N, Lycke H. Effects of vocal training on singing and speaking voice characteristics in vocally healthy adults and children based on choral and nonchoral data. J Voice. 2011 Jul;25(4): e177-89.
- Sheikh JI, Yesavage JA. Geriatric Depression Scale (GDS). In: Brink TL. Binghamton NY, eds. Clinical Gerontology. New York: Haworth Press; 1986:165–173.
- Hirano M. Clinical examination of voice. New York: Springer Verlag, 1981.
- Santos SB, Rodrigues SR, Gadenz CD, Anhaia TC, Spagnol PE, Cassol Ma. Verifying the effectiveness of using resonance tubes in voice therapy with elderly people. Audiol Commun Res. 2014; 19(1):81-7
- Wang CC, Chang MH, Jiang RS, Lai HC, Virgilio A, Wang CP, Wu SH; Liu SA; Liang KL. Laryngeal Electromyography-Guided Hyaluronic Acid Vocal Fold Injection for Unilateral Vocal Fold Paralysis - A Prospective Long-term Follow-up Outcome Report. JAMA Otolaryngol Head Neck Surg. 2015;141(3):264-271. Available in: http://dx.doi.org/10.1001/jamaoto.2014.3466
- Clift SM, Hancox G. The perceived benefits of singing: findings from preliminary surveys of a university college choral society. J R Soc Promot Health. 2001;121(4):248-56.
- Cohen GD, Perlstein S, Chapline J, Kelly J, Firth KM, Simmens S. The Impact of Professionally Conducted Cultural Programs on the Physical Health, Mental Health, and Social Functioning of Older Adults in 2 Year Results. Journal of Aging, Humanities and the Arts. 2007; 1:5–22.
- Skingley A, Martin A, Clift S. The Contribution of Community Singing Groups to the Well Being of Older People Participant Perspectives From the United Kingdom. Journal of Applied Gerontology, Published online before print March 23, 2015. [captured 2015 May 05]; 2015. Available in: http://dx.doi.org/10.1177/0733464815577141
- Hays T, Bright R, Minichiello R. The Contribution of Music to Positive Aging: A Review. Journal of Aging and Identity. 2002; 7:165–175.
- Bilton, T.; Viúde, A. E Sanchez, E. P. Fonoaudiologia. In: Gorzoni, M. L. & Rocha, S. M. Tratado de Geriatria e Gerontologia. Rio de Janeiro: Guanabara Koogan, 2002. p. 821
- Hara S, Miura H, Yamasaki K, Morisaki N, Osaka K. Relationship among Subjective Satisfaction with Verbal Communication, Dental Status, and Health-Related Quality of Life in Japanese Community-Residing Elderly Individuals. Advances in Applied Sociology. 2015; 5:32-39. Available in: http://dx.doi.org/10.4236/aasoci.2015.51004
- Li HC, Wang HH, Chou FH, Chen KM. The Effect of Music Therapy on Cognitive Functioning Among Older Adults: A Systematic Review and Meta-Analysis. JAMDA. 2015; 16:71-77. Available in: http://dx.doi.org/10.1016/j.jamda.2014.10.004



