Public Health and Preventive Medicine, Vol. 1, No. 2, June 2015 Publish Date: May 28, 2015 Pages: 62-65
Health Care Practices among the Dimasa Tribe of Diyungbra Block in Dima Hasao District, Assam
Mili Bodo1, Bhaskarjyoti Bodo2, *
1Department of Education, Thong Nokbe College, Dokmoka, Assam, India
2Department of Physics, Diphu Govt. College, Diphu, Assam, India
Abstract
In our present work, health care practices among the indigenous Dimasa tribe of Diyungbra block, Dima Hasao District, Assam were studied. In the study, it was observed that health care consciousness had been spreading among them very rapidly. It is because of the educational development and of easy access to the relevant information through print as well as electronic media. Moreover, the flagship programme on health care awareness initiated by government and NGO contributed to the mass education in the field of health care and the benefit from such activities even penetrated to the illiterates. Consequently numerous superstitious beliefs and evil practices on the diseases have been declined drastically. Thus a dynamic transition phase in their health care system was observed. Another important finding is their ethnomedical use in some diseases. Such traditional knowledge and dexterous skills of using medicinal plants and herbs profusely found in the habitat of Assam have been evolved since time immemorial and have been perpetuated generation to generation among these indigenous Dimasa People as hierarchy. So, there is a great demand on scientific investigations on the efficacy of using such plants and herbs on curing some diseases and it will attract the great attention of scientific communities in the field of medicare and medicine.
Keywords
Ayurvedic, Dimasa, Ethnomedicinal Plants, Health Care, Etc
Received: April 7, 2015
Accepted: April 23, 2015
Published online: May 27, 2015
@ 2015 The Authors. Published by American Institute of Science. This Open Access article is under the CC BY-NC license. http://creativecommons.org/licenses/by-nc/4.0/
1. Introduction
Health care is an increasing important policy area in today’s global society and it is rapidly growing economic sector in the world [1]. Many research scholars are pursuing research works in this field and they claim that it is very difficult to predict what the facilities the future hospital will be equipped with [2]. The reinvention of health care is very complex [2-3] and its implication is more tedious jobs with various social constraints and taboos.
It is well known that the area of tribal settlement are in need of social and health programme those provide them with even basic protection from infectious diseases such as from bacteria and viruses[4]. Of course in the recent times with increase knowledge of life and culture of the tribal communities, the health care among themselves have changed drastically [5]. Many Research Scholars carried out ethno-medical beliefs and practices prevalent among the tribal communities of Assam in India [6-8]. In this study an humble attempt has been made to investigate the interrelationships among health care, economic and educations of the Dimasa people of Diyungbra Block in the District of Dima Hasao, Assam, India.
2. The Dimasa Tribe
The Dimasa is a scheduled Tribe in the Autonomous Hills district, Dima Hasao of Assam in India and their sizeable population are found in the neighbouring districts such as Nagaon, Karbi Anglong, Chachar and Hailghandhi [5,9]. They belong to the Bodo tribes which include Bodo, Kacharis, Rabha, Lalung, Tripurah, Tiwa, Mech and Sonowal [10].
The name Dimasa is derived from the river "Dima" (Dansri) of Dansri valley in the Karbi Anglong District, Assambordering Nagaland and ‘Sa’ means son thus meaning the son of the river Dima [11]. These people were known as Bodosa prior to their settlement in Dansri valley with Dimapur as the capital of Kachari Kingdom. Once they started to domicile there they came to be known as Dimasa [5,10,11].
3. Materials and Method
3.1. The location of Study
Assam is situated in the north east corner of India. The state is located between 900-960 East latitude and 220-280 North latitude [12]. Dimasa Hasao district is situated southern part of Assam while Diyungbra block is located in the northern part of Dima Hasao district bordering the northern part of west Karbi Anglong district. More over the location of the study is within about 18 km from the Lanka town of Nagaon district in Assam. There are different communities domiciled in the Diyungbra block but the Dimasa population is majority in this area. The inhabitants of Diyungbra block get many facilities such as medical, education, marketing etc at the Lanka town in the district of Nagaon, Assam. They can easily communicate to other places through railway station at Lanka and by road transportation.
3.2. The Livelihood of Dimasa Tribe
The majority of the Dimasa tribe of the Diyungbra and of its adjoining villages are dependent mainly on agricultural activities throughout the year. While men remains busy in outdoor agriculture and allied activities, women folk also indulge themselves in maintaining the household activities like cooking, bringing water, rearing poultry, weaving cloths, collecting fire wood [5,9]. The children above 10 years are also used to work in domestic works. The aged men and women also assist the young household members in various activities such as looking after the young children, doing cane and bamboo works and other petty jobs which do not require physical exercises. Thus in the rural tribal area it is very difficult to distinguish among the earners and the non-earners [9]. The women folk are expertise in weaving the cloths and they rear the poultry while the women folk who are casual earners depending upon the head of the household and help partially agricultural activities may be considered as earning dependent[5].
3.3. Methodology and the Sample of the Study
The community based survey was carried out among the Dimasa people of Diyungbra block in the district of Dima Hasao, Assam in India. The selection of the samples of the study was entirely based on the concentration of the tribal and a stratified strategy was adopted to choose the sample [4]. All the household members above the 18 years were eligible to participate following voluntary consent. The table:1 represents the numbers of participant from the location of our study.
Table 1. The sample of the study:
| Sl.no | Village | Population | Literacy rate (%) | ||
| Male | Female | Total | |||
| 1 | Rajbari | 126 | 120 | 246 | 75% |
| 2 | Baraima | 105 | 102 | 207 | 57.9% |
| 3 | Chotowashling | 95 | 88 | 183 | 71% |
| 4 | Probdisa | 96 | 102 | 198 | 68.2% |
| 5 | Washibil | 83 | 91 | 174 | 63.7% |
The participants were randomly selected and the survey questionnaires were individually administered to them. These questionnaires were designed on the basis of multiple choice questions as well as yes/no responses depending upon the need of particular information. This survey included demographic information such as age, ethnicity, level of education, occupation and house hold income and their health care consciousness in particular.
4. Results and Discussion
Wide spread poverty, illiteracy and malnutrition, lack of personal hygiene, scarcity of drinking water, sanitary, living conditions and health education, insufficient maternal and child health services and inadequate coverage by the national health and nutritional services have been identified as conditions responsible for poor health status of the Dimasa people of the Dima Hasao district[4]. Their settlement tends to be small and isolated and difficult to reach with facilities and services. Even when rural tribal people live in larger villages they may be separated in hamlets. However these tribal people are relatively well integrate into communities and their social set up is strongly organized [2]. This strong social web plays an important role on rapidly spreading of the enlightenment of basic education and the health consciousness among the Dimasa people very fast.
In the contest of the people of Diyungbra, they have certain advantages in their livelihoods due it strategic location and abundance of agricultural lands compared to the other part of the Dima Hasao District [5]. The sound pecuniary conditions of the household make them access to modern medical facilities which are available in its close proximity. Moreover, the flagship programme on health care awareness initiated by government and NGO contributed to the mass education in the field of health care and the benefit from such activities even penetrated to the illiterates. Consequently numerous superstitious beliefs and evil practices on the diseases have been declined drastically.
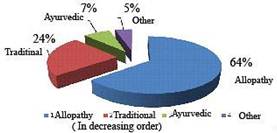
Figure 1. Preferance wise distribution of medical treatments
In our study it was found that the 64% of the Dimasa people preferred to approach the doctor for medical treatment, 24% of those population followed traditional health care and the 7% of the people used the Ayurvedic medicine and the rest followed alternative methods [10] as shown in figure-1. When data collected were classified into the populace of the literate and illiterate, there was clear indication that literate people are more aware about the modern system of therapeutic treatment. The uses pattern of different medical treatments on the basis of the literates and illiterates are depicted in figure-2.
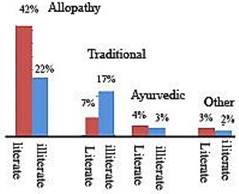
Figure 2. The comparison of the preference of different medical treatments among the litterate and illiterate people
Table 2. Some medicinal plants used by the Dimasa people of Diyungbra block of Dima Hasao District, Assam:
| Dimasa name | Plants name | Family | Uses |
| Sinju | Achyranthes aspera L | Amaranthaceous | Crushed leaves are used to cure cramps and piles |
| Sermuli | Aegle Marmelos Correa | Rutaeceae | Fruit is taken in case of asthma, constipation and dysentery, leaf extract is taken to cure jaundice |
| Alumikhri | Begonia roxburghii A. | Begonaiaceae | Paste of rhizome is taken for malaria; stem extract is used in cough&pneumonia |
| Waigolai | Bryophyllum CalycinumSalib | Crassulaceae | Crushed leaves are applied on burns and bruises; leaf extracts is used to remove the kidney stones. |
| Dukhakhun | Cascuta Reflexa Roxb | Convolvulaceae | Whole plant extract is used for the treatment of jaundice and premature graying of hair |
| Morsaidi | Pipper nigrum L. | Piperaceae | Crushed seeds are used to cure pneumonia and cough; root extract is taken in dysentery and piles. |
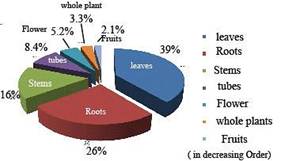
Figure 3. Percentage wise use of different parts of medicinal plants in ethnomedical treatment among the Dimasa people
Though the worshiping of supernatural power with sacrifice of animals has been remarkably abated, the traditional uses of ethnomedicinal plants are still pervaded among the Dimasa people of Diyungbra like other tribal do [13-14]. Some of such medicinal plants are listed in table-2. The cross examinations of the different parts of the medicinal plants are depicted in the figure-3. Our finding in this regard suggests that the ethnomedicinal plants in the treatment of various diseases still play an important role in their society [14].
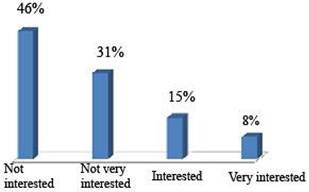
Figure 4. Reported responses of the different level interest of the new generations age between 18years and 30 years.
To know the importance and uses of these ethno-medicinal plants among the new generations, the surveys with different level of interest were carried out among 125 peoples; the ages ranging from 18 years to 30 years. The figure-4 represents such randomly collected data clearly indicating that majority of them were not much interest in such system of health care. If this trend continues in the new generation the ehtnomedical treatment, the poor man’s medicine will be in the state of extinct. Therefore, scientific research on such medicinal plants should be given the utmost priority for the revivals of its value and importance so that it becomes more acceptable for all [14].
5. Conclusion
The synergetic effect of health care consciousness on educational development as well as economic uplift among the Dimasa tribe of Diyungbra block and their inter-relationships in particular were promptly observed in this study. Though majority people preferred for modern medical facilities for therapeutic treatment the ethnomedicinal plants in the treatment of various diseases still play an important role in their society. So the scientific research on such medicinal plants should be given the utmost priority for the revival of its value added importance and usefulness in the society.
Acknowledgement
Authors sincerely thank Dr Rajesh Rongpi M D, Diphu Civil Hospital, Diphu, and Mr SanjibTarafdar, Assam Institute of Research Centre for ST/SC, for their assistance and valuable suggestions in carrying out the survey.
References
- Sagar, Renuka; Praveena, P. Lalitha, An Analytical study of FDI in Indian Health care sevtor, International Journal of Social Science and Interdisciplinary Researc.2013, 2(8) , 29-38.
- Bricon-Souf, Nathalie; Newman, Conrad R. Context in health care: A review, International Journal of Medical Informatics, 2007, 76(1), 2-12.
- Coiera, E. Four rules for the reinvention of health care, BMJ, 2004, 328, 1197-1199.
- Talukdar, Simi; Gupta, Abhik, Medical Plants used by the Bodo community of Chakrashila Wildlife Sanctuary, Assam , India, Indian Journal of Applied Research, 2014, 4 ,1-4.
- Bodo, Mili,(2009) Impact of female literacy on socio-economic development of the Dimasa people, Diyungbra block, unpublished M Phil thesis, Vinayak Mission University, Salem , Tamil Nadu.
- Tamuli, P.; Sarma, P.Eethino- medico botany of the DimasaKachari of North Cachar Hills district of Assam, Indian Journal of Traditional knowledge, 2010, 9(4), 718-720.
- Das, Ajit Kumar. et al, Medicinal plants used by different tribes of Cachar district, Assam, Indian Journal of Traditional knowledge, 2008,7 (3) , 446-454.
- Albert, L S; Gosai,Kuldip, Traditional use of medicinal plants by the Jaintia tribes in North Cachar Hills of Assam, Northeast , Indian Journal of Ethnology and Ethomedicine, 2006,2.33.
- Bordolloi B. N., TheDimasaKacharis of Assam, Tribal Research Institure, Assam, 1984.
- Gait, E.A, A History of Assam (Reprint) Guwahati University,1968.
- Bodo,K. C.,Dimajaji Harang Gaodhu (The erosion of Dimaraji), Tribal cultural centre, Lanka 1982.
- Dilip,Kalita, Dilip; Phukan, Bonoronjan, Some ethnomedicines used by the Tai Ahom of Dibrugarh district , Assam, India, IndianJournal of Natural Products and Resources, 2010, 1(4) , 507-511.
- Varadarajan, Y Ltekhre;Sarma,Alka ,Indigenous Health practices among AndraTrabals, Health and population: Prospective and Issues,2009,32(1), 47-53.
- Pushpangadan,P.;George, V.,Ethnomedical practices of rural and tribal populations of India with special reference to the mother and childcare, Indian Journal of traditional Knowledge, 2010, l 9(1), 9-17.



