
American Journal of Clinical Neurology and Neurosurgery, Vol. 1, No. 2, September 2015 Publish Date: Aug. 5, 2015 Pages: 74-76
Giant, Ventral, Cervical Spinal Neurenteric Cyst Presenting with Acute-Onset Quadriparesis – Surgical Management and Discussion
Ribhav Pasricha, Guru Dutta Satyarthee*, Bhawani Shankar Sharma
Department of Neurosurgery, All India Institute of Medical Sciences, New Delhi, India
Abstract
A giant, ventrally placed cervical spinal neurenteric cyst in a pediatric patient presented with acute onset quadriparesis. Magnetic resonance imaging showed a large cyst in the cervical spine lying ventral to the cord at C2-C3 levels and causing severe cord compression. Cyst decompression surgery involved laminoplasty, cyst drainage and wall excision with minimal cord retraction. The procedure resulted in immediate improvement of muscle power in all four limbs of the patient. Ventrally placed intradural lesions in the cervical spinal cord can be a surgical challenge and the decision between the appropriate anterior or posterior approach should be made on the individual patients clinical and radiological profile.
Keywords
Pediatric Spinal Tumors, Spinal Tumors, Neurenteric Cyst, Laminoplasty, MRI
Received: July 15, 2015
Accepted: July 25, 2015
Published online: August 4, 2015
@ 2015 The Authors. Published by American Institute of Science. This Open Access article is under the CC BY-NC license. http://creativecommons.org/licenses/by-nc/4.0/
Contents
1. Case Report
A 9- year old girl presented to the emergency department with acute onset rapidly progressive quadriparesis for the last 20 days. The patient was conscious and obeying commands. Both her upper limbs were in a state of complete flaccid paralysis with muscle power of 0/5. Her lower limbs had spastic paraparesis with muscle power of 2/5 (Medical Research Council scale, United Kingdom). Her knee and ankle jerks were 2+, while all the other deep tendon jerks were diminished or absent. Her plantars were upgoing (Babinski sign positive). The patient’s MRI showed a large cystic lesion of the cervical spine lying ventral to the cord at C2-C3 levels and causing severe cord compression. T2w images showed homogeneous hyperintensity and postcontrast images showed no enhancement of the cyst wall (figure 1). These features were suggestive of a giant, ventral, cervical neuroenteric cyst.
The patient was operated upon with a C2-C3 laminoplasty and cyst fenestration. Following dural opening, the cord was gently retracted to one side to expose the cyst, lying ventral to it. The cyst wall was smooth and fleshy and greyish in colour (figure 2). Blood stained clear fluid was drained from the cyst, and the cyst wall lining was sent for histology with a suspicion of neuroenteric cyst. The cord was well decompressed at the end of surgery. Postoperatively, the patient’s muscle power improved in her right upper and lower limbs on the first day itself upto 3/5 (Medical Research Council scale). Her plantars became equivocal and the spasticity in her lower limbs decreased.
2. Discussion
Neurenteric cysts are rare congenital lesions found intracranially and in the spine. They result from an anomalous persistence of the endodermal - neuroectodermal canal and hence are lined with endodermal epithelium [10]. Their most common location in the spine is the cervico-dorsal region although lumbar and rarely presacral locations have also been seen [1,2,6]. They are usually intradural extramedullary although they may be intramedullary also[11]. They usually lie ventral to the spinal cord. Associated vertebral anomalies, gut cysts, bowel duplication, the presence of keratin markers and mucin-secreting cuboidal or columnar intestinal epithelium in their walls confirm their endodermal origin [3,4,5]. This was a rare case in which a giant intraspinal cyst was present without any associated vertebral anomalies or other systemic findings (figure 3). For ventrally placed lesions in the cervical spinal cord, both anterior and posterior approaches have been described [7,8,12]. Posterior approaches with gentle cord rotation may provide adequate exposure for safe removal of ventrally placed spinal cord lesions, as in the index case. However in certain cases, anterior approaches become necessary especially in ventrally placed midline lesions where excessive cord traction from a posterior approach would entail risk of development of neurological deficits in the patient [9].
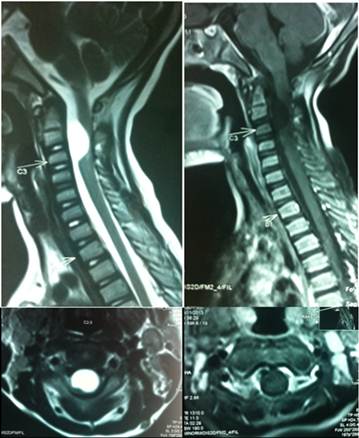
Figure 1. MRI images showing an iso-intense with CSF, intradural extramedullary ventral cystic mass at C2-C3 level. a – T2w sagittal, b – postcontrast T1w sagittal, c- T2w axial, d – postcontrast T1w axial.
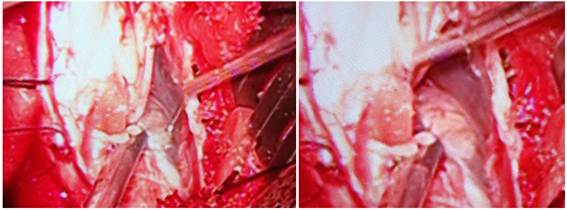
Figure 2. Intraoperative image showing cord pulled to one side and greyish cyst wall of the giant neuroenteric cyst.

Figure 3. 3 a-Preoperative T1w MRI image showing severe cord compression, 3b- T2w screening image of the whole spine showing no other abnormalities.
3. Conclusion
Spinal neurenteric cysts are usually ventrally located intradural lesions that pose a surgical challenge for their safe removal while minimising risk of postoperative deficits. Lesions off the midline can be safely removed using a posterior approach by ensuring wide exposure and gentle traction on the cord. With adequate decompression, surgical results are excellent and operated patients show an immediate improvement in limb power.
References
- Satyarthee GD, Mahapatra AK. Presacral neurenteric cyst in an infant. Pediatr Neurosurg. 2003 Oct;39(4):222-4.
- Rodrigues D, Behari S, Ismail A, Crawford P. Giant presacral neurenteric cyst with anomalous sacrum in an adult patient. Br J Neurosurg. 2005 Apr;19(2):181-4.
- Kumar R, Jain R, Rao KM, Hussain N. Intraspinal neurenteric cysts--report of three paediatric cases. Childs Nerv Syst. 2001 Oct;17(10):584-8.
- Wakisaka M, Nakada K, Kitagawa H, Shimada H, Nosaka S. Giant transdiaphragmatic duodenal duplication with an intraspinal neurenteric cyst as part of the split notochord syndrome: report of a case. Surg Today. 2004;34(5):459-62.
- Zhang F, Lu G. Giant mediastinal neuroenteric cyst with intraspinal neurenteric cyst. Eur J Radiol. 2008 Nov;68(2):e59–e61.
- Jhawar SS, Mahore A, Goel A. Intramedullary spinal neurenteric cyst with fluid-fluid level. J Neurosurg Pediatr. 2012 May;9(5):542-5.
- Sasani M, Ozer AF, Oktenoglu BT, Peker K, Bozkus MH, Sarioglu AC. Excision of an asymptomatic cervical intradural neurenteric cyst through the anterior approach: a study of two cases and a review of the literature. Spine J. 2007 Nov-Dec;7(6):720-7. Epub 2007 Feb 20.
- Tuzun Y, Izci Y, Sengul G, Erdogan F, Suma S. Neurenteric cyst of the upper cervical spine: excision via posterior approach. Pediatr Neurosurg. 2006;42(1):54-6.
- Angevine PD, Kellner C, Haque RM, McCormick PC. Surgical management of ventral intradural spinal lesions. J Neurosurg Spine. 2011 Jul;15(1):28-37.
- Cai C, Shen C, Yang W, Zhang Q, Hu X. Intraspinal neurenteric cysts in children. Can J Neurol Sci. 2008 Nov;35(5):609-15.
- Yang T, Wu L, Fang J, Yang C, Deng X, Xu Y. Clinical presentation and surgical outcomes of intramedullary neurenteric cysts. J Neurosurg Spine. 2015 Jul;23(1):99-110.
- Laidlaw JD. Iso-intense neuroenteric cyst in the lower cervical spine treated with ventral resection and anterior fusion utilising sternal notch exposure: case report, technical note and literature review. J Clin Neurosci. 2003 Sep;10(5):606-12.



