
American Journal of Clinical Neurology and Neurosurgery, Vol. 1, No. 2, September 2015 Publish Date: Aug. 6, 2015 Pages: 92-98
Knowledge and Practice of ICU Nurses Regarding Endotracheal Suctioning for Mechanically Ventilated Patients in Khartoum Teaching Hospital
Raghda Elbokhary1, *, Await Osama2, Mugahed AL-khader1
1Medical Surgical Nursing Department, Faculty of Nursing, Sudan International University, Khartoum, Sudan
2Department of Anesthesia, University of Medical Science and Technology, Khartoum, Sudan
Abstract
Study purpose: The aim of this study is to assess knowledge and practice of ICU nurses regarding mechanically ventilated patients endotracheal suctioning in Khartoum teaching hospital. Methods: This is a descriptive cross-sectional hospital based study. A total coverage (42 nurses) sampling technique was used to select nurses. All nurses working in Khartoum teaching hospital ICU included in the study. Result: the majority of nurses working in Khartoum teaching hospital (35.7%) have 2 mon-1 year working experience, (85.7%) have poor knowledge level, (76.7%) have fair practice level, and there is no significant relationship between working experience & levels of knowledge & practice. Conclusion: Nurses have better practical level than knowledge level and they were not affected by nurse’s length experience as there should be.
Keywords
Knowledge, Practice, ICU Nurses, Endotracheal Suctioning, Mechanical Ventilation
Received: July 10, 2015
Accepted: July 20, 2015
Published online: August 6, 2015
@ 2015 The Authors. Published by American Institute of Science. This Open Access article is under the CC BY-NC license. http://creativecommons.org/licenses/by-nc/4.0/
Contents
1. Introduction 2. Materials and Methods 3. Result 3.1. Knowledge of ICU Nurses Regarding Mechanically Ventilated Patients Endotracheal Suctioning in Khartoum Teaching Hospital 3.2. Practices of ICU Nurses Regarding Mechanically Ventilated Patients Endotracheal Suctioning in Khartoum Teaching Hospital 4. Discussion
1. Introduction
Endotracheal suctioning (ETS) is one of the most common procedures performed in patients with artificial airways. It is a component of bronchial hygiene therapy and mechanical ventilation that involves the mechanical aspiration of pulmonary secretions from a patient’s artificial airway to prevent its obstruction. The procedure includes patient preparation, the suctioning event, and follow-up care (1).
Endotracheal suctioning (ETS) is a process in which the catheter inserted in to the endotracheal tube and the secretions of patient’s lung removed with applying the negative pressure. This process prevents accumulation of the secretion, thereby maintains airway patency and ensures optimal oxygenation and saving the patients’ lives. However, failure to meet the standards in the implementation of this procedure can have numerous detrimental effects. Possible complications of endotracheal tube suctioning include hypoxia, bronchospasm, atelectasis, tracheal tissue injury, ventilator-associate pneumonia, increase in intracranial pressure, and cardiac dysrhythmia. All intensive care nurses should be aware when performing this intervention of the potential hazards a patient is exposed to, and should Endeavour to prevent or minimize these. Therefore, updating endotracheal tube suctioning practices is considered to reduce the incidence of these complications. (2)
ETS is probably one of the most common invasive procedures performed in patients with an artificial airway (2). It’s also described by patients as painful and uncomfortable, and may result in chocking sensation initiating a violent cough, and also cause an unpleasant sensation that the lungs are actually being suctioned into the catheter (3). Despite the discomfort, patients report that the procedure is necessary and subsequently eases their breathing. The discomfort associated with suctioning does not diminish during the course of mechanical ventilation; on the contrary it may worsen. (4)
Suctioning for intubated and ventilated patients is a routine nursing procedure, yet practices vary among clinicians and hospitals. Some suctioning practices which have little to no evidence to support their use are still being performed. It must be recognized that a lack of research evidence does not necessarily mean that a practice is of no benefit. Alternatively, there may be some practices that continue even when strong evidence clearly indicates either no benefit or actual harm. Invasive techniques such as manual ventilation with a bag-valve-mask and instillation of normal saline have been shown to have no benefit to the patient when suctioning yet despite this, these practices continue in some Units. (5)
Endotracheal suctioning is a sterile procedure that nurses must perform efficiently and effectively in order to avoid infections. nurses lack of adherence to aseptic technique is a factor in transmitting infection or cross infection which in turn increases patients length of stay and prone the patients to more and more risk of infection
Mechanical ventilation is widely used for critically ill patients. Endotracheal suctioning is the necessary procedure carried out in the intensive care units but has a number of potential risks and complications that ranges from hypoxemia to cardiac rhythm disturbances, trauma, and in extreme circumstances cardiac arrest and death. Patients may also experience moderate to severe pain. Ventilator associated pneumonia is the major complication. It is therefore imperative that healthcare professionals are aware of these risks and are able to practice according to current best evidence.
Researchers have identified that nurses are unaware of current suctioning recommendations and practice is often based on ritual and tradition as opposed to empirical. Nurse’s lack of adherence to aseptic technique may be a factor in transmitting infection or cross infection which in turn increases patient’s length of stay. When an infection can be prevented by ordinary and reasonable care, nurses must use such care. Adequate knowledge along with the correct procedure performance is required to follow the aseptic technique which in turn prevents infection. So it’s imperative to assess their knowledge and practice level for endotracheal suction.
The scientific knowledge on which nurses base their clinical practice is often lacking. Nurse’s lack of adherence to aseptic technique may be a factor in transmitting infection or cross infection. When an infection can be prevented by ordinary and reasonable care, nurses must use such care. Adequate knowledge is required to follow the aseptic technique. (8, 9)
This study will also help to put ground and identify knowledge gaps pertaining endotracheal suctioning in order to close those gaps for better patient outcome.
And because nurse’s knowledge and practice estimation here in Sudan is not reported, the result is increase rate of morbidity and infection for ventilated patients.
Unless, nurses knowledge and practice level is identified; minimizing ventilator associated pneumonia and other complications is difficult to be achieved.
From this we conclude that assessment of nurse’s knowledge and practical experience regarding proper endotracheal suctioning is crucial in order to perform suction procedure with efficiency.
2. Materials and Methods
This is a descriptive cross-sectional hospital based study. This study used a descriptive approach to assess nurse’s knowledge and practice. The study was conducted in Khartoum Teaching Hospital ICU. Khartoum teaching hospital was established 1964, which lies in Khartoum city, and is the capital of Sudan. It has the largest number of patients coming from all different Khartoum localities and occasionally from other states. Khartoum teaching hospital has 2 intensive care units with a maximum of 10 beds for both.
The study will be conducted on all ICU nurses caring for adult mechanically ventilated patients with endotracheal tube in Khartoum teaching hospital. The study included post graduate, bachelor holders, registered nurse. The study did not include the nurses who refused to participate in the study.
The data for this research was collected using a designed structured questionnaire and observational check list as tool for data collection. The data was collected from nurses by the researcher during their working time in duty. The researcher attended all the nurses’ duties in order to collect accurate data. Questionnaires were filled by nurses while the check list was filled by the researcher during observing nurses while performing the procedure.
Total coverage technique is used to include all 42 nurses working in Khartoum teaching hospital ICU,and the data is analysed by using SPSS package and the results is showed in figures, graphs and tables that contains frequency and percentage of the result findings. The data is analysed using a chi-square test as a procedure to analyse the findings.
The level of knowledge was ranked into three levels; more than (75%) are good knowledge, (50-75 %) are fair knowledge, and less than (50%) are poor knowledge, and the level of practice was ranked into three levels; more than (75%) are good practice, (50-70 %) are fair practice , and less than (50%) are poor practice.
The research is respecting the rights of participants, treat data with confidentiality no harm for the subject. All study participants is provided with a written consent prior to participation in the study. Approval from University of Medical Sciences and Technology – Faculty of Nursing Sciences is taken. Permission from study area is taken (Khartoum teaching hospital).
3. Result
3.1. Knowledge of ICU Nurses Regarding Mechanically Ventilated Patients Endotracheal Suctioning in Khartoum Teaching Hospital
Table 1. Distribution of ICU nurse’s according to their knowledge regarding mechanically ventilated patients endotracheal suctioning in Khartoum teaching hospital.
| Knowledge questions | Right answers | Frequency | percent |
| definition of M.V | Life support system | 37 | 88.1 % |
| Indication for M.V | Respiratory Failure | 30 | 71.4% |
| Assessment of M.V Patient | Auscultating breath sounds every hour | 13 | 31.0% |
| Prevention of the risk of pneumonia in M.V.P | Chest physiotherapy | 34 | 81.0% |
| Assessment for ETS | Visible or audible secretions | 27 | 64.3% |
| Exception for Auscultation for the need of ETS | Wheezing | 20 | 47.6% |
| Oxygenation monitoring technique | Monitoring the arterial blood gases | 18 | 42.9% |
| Definition of ETS | Removal of secretions from an artificial airway | 20 | 47.6% |
| exception for Indications of ETS | Murmurs | 22 | 52.4% |
| Prevention of nosocomial infections | Wash hands and maintain aseptic technique | 20 | 47.6% |
| Size of ETS catheter | Less than half the internal diameter of the tracheal tube | 27 | 64.3% |
| Effect of Preoxygenation in ETS | It minimizes hypoxia | 27 | 64.3% |
| Recommended time duration for ETS | 10-15 seconds | 19 | 45.2% |
| ETS source pressure | 80-120 mmhg | 19 | 45.2% |
| ETS frequency | Only when clinically indicated | 26 | 61.9% |
| exception for Complications of ETS | Decreased blood volume | 19 | 45.2% |
| Contraindications for ETS | Both pts with an increased intracranial pressure & pt with severe HTN | 6 | 14.3% |
| Adverse effects of ETS | Reduction in lung volume | 6 | 14.3% |
| Normal Saline instillation during ETS | Not recommended | 6 | 14.3% |
| effect normal Saline instillation | All Tachycardia, dyspnea and VAP | 18 | 42.9% |
| Effect of increased ETS frequency | Atelectasis | 7 | 16.7% |
| the reason behind discontinuation of procedure | Heart rate is above or below normal level and cardiac ectopy | 6 | 14.3% |
| exception for adverse effects of hyperinflation | Decrease cardiac output | 6 | 14.3% |
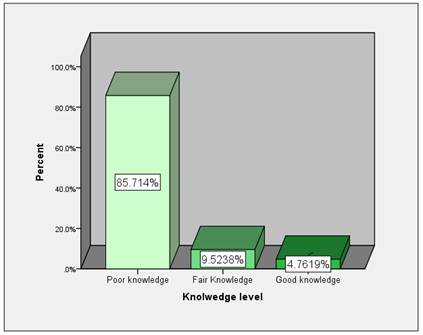
Figure 1. distribution of nurses according to their knowledge level in Khartoum teaching hospital 2014.
3.2. Practices of ICU Nurses Regarding Mechanically Ventilated Patients Endotracheal Suctioning in Khartoum Teaching Hospital
Table 2. Distribution of nurses according to their actions by using Observation checklist to assess the practical level of ICU nurses regarding ETS.
| Item | Done | Not done | |||
| Freq. | Percent | Freq. | percent | ||
| 1. preparatory phase: | |||||
| 1 | Assemble equipment. | 21 | 70.0 | 9 | 30.0 |
| 2 | Check function of suction apparatus | 30 | 100.0 | 0 | 00.0 |
| 3 | Monitor heart rate. | 30 | 100.0 | 0 | 00.0 |
| 4 | Record blood pressure. | 30 | 100.0 | 0 | 00.0 |
| 5 | Monitor oxygen saturation. | 21 | 70.0 | 9 | 30.0 |
| 6 | Auscultate breath sounds. | 0 | 00.0 | 30 | 100.0 |
| 2. performance phase: | |||||
| 7 | Explain the procedure to the patient. | 8 | 26.7 | 22 | 73.3 |
| 8 | Position the patient in fowler’s position. | 16 | 53.3 | 14 | 46.7 |
| 9 | Wear the face mask. | 6 | 20.0 | 24 | 80.0 |
| 10 | Wash hands with antimicrobial agents. | 16 | 53.3 | 14 | 46.7 |
| 11 | Have an assistant to help with the procedure. | 18 | 60.0 | 12 | 40.0 |
| 12 | Place the sterile towel on the patient’s chest/bed table | 0 | 00.0 | 30 | 100.0 |
| 13 | Open sterile gloves. | 24 | 80.0 | 6 | 20.0 |
| 14 | Place the sterile gloves on the towel/bed table. | 0 | 00.0 | 30 | 100.0 |
| 15 | Put on the sterile gloves; designate one hand as clean (non-dominant hand). | 30 | 100.0 | 0 | 00.0 |
| 16 | Keep the dominant hand sterile to thread the suction catheter | 16 | 53.3 | 14 | 46.7 |
| 17 | Ask the assistant to open the suction catheter. | 28 | 93.3 | 2 | 6.7 |
| 18 | Ask the assistant to pour normal saline into the bowl. | 12 | 40.0 | 18 | 60.0 |
| 19 | Use the sterile hand to remove the suction catheter. | 30 | 100.0 | 0 | 00.0 |
| 20 | Ask the assistant to disconnect the patients from the ventilator. | 17 | 56.7 | 13 | 43.3 |
| 21 | Ask the assistant to hyper oxygenate the patient before suctioning using ambu-bag increasing FIO2 to 100%. | 8 | 26.7 | 22 | 73.3 |
| 22 | Gently but quickly insert catheter into artificial way using sterile/ dominant hand. | 16 | 53.3 | 14 | 46.7 |
| 23 | Don’t apply suction while inserting catheter. | 18 | 60.0 | 12 | 40.0 |
| 24 | Pull back the catheter 1-2 cm if resistance is met | 16 | 53.3 | 14 | 46.7 |
| 25 | Apply suctioning by placing and releasing the dominant thumb on the vent of the catheter | 20 | 66.7 | 10 | 33.3 |
| 26 | Withdraw the catheter while rotating it back | 16 | 53.3 | 14 | 46.7 |
| 27 | Limits suction time to 10-15 seconds. | 10 | 33.3 | 20 | 66.7 |
| 27 | Discontinue if heart rate is below or above normal. | 24 | 80.0 | 6 | 20.0 |
| 28 | Asks the assistant to return the patient to the ventilator. | 22 | 73.3 | 8 | 26.7 |
| 29 | Rinse the catheter and connecting tube with normal saline until clear. | 24 | 80.0 | 6 | 20.0 |
| 30 | Assess patient’s cardiopulmonary status. | 6 | 20.0 | 24 | 80.0 |
| 31 | Assess for secretion clearance. | 6 | 20.0 | 24 | 80.0 |
| 32 | Don't perform more than 4suction per suctioning. | 14 | 46.7 | 16 | 53.3 |
| 33 | Don't reinsert the suction catheter into endotracheal tube. | 16 | 53.3 | 14 | 46.7 |
| 34 | Discard gloves. | 30 | 100.0 | 0 | 00.0 |
| 35 | Turn off the suction device. | 30 | 100.0 | 0 | 00.0 |
| 36 | Perform hand hygiene. | 30 | 100.0 | 0 | 00.0 |
| 37 | Note any changes in the vital signs. | 0 | 00.0 | 30 | 100.0 |
| 38 | Document the procedure. | 0 | 00.0 | 30 | 100.0 |
| 39 | Wash and replace the articles. | 0 | 00.0 | 30 | 100.0 |
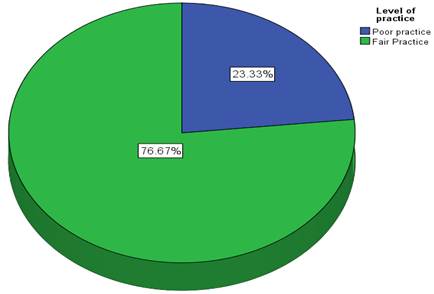
Figure 2. Distribution of total practice level for ICU nurses in Khartoum teaching hospital.
4. Discussion
This descriptive crossectional hospital based study was carried on Khartoum teaching hospital ICU nurses. The study included a total of 42 nurses which is the total number of ICU nurses working in Khartoum teaching hospital 2014.
This study’s general objective aimed to assess Khartoum teaching hospital ICU nurses knowledge and practice regarding endotracheal suction for mechanically ventilated patients by using a structured questionnaire and check list. The questionnaire used was a single best answer and it was divided into 3 sections, which are the specific objectives, and they were: assessment of nurse’s knowledge regarding ETS practice, assessment of nurse’s practice regarding ETS performance and exploration of the relationship between working experience and levels of knowledge and practice.
Working experience of all Khartoum teaching hospital ICU nurses was assessed. This study showed that the majority of nurses 35.71% have a working experience from 2mon-1year. While only 21.4% worked there for more than 3 years.
One of the study objectives, in order to assess nurse’s knowledge, was regarding nurse’s assessment for MVP (table.1). This study revealed that 88.1% of nurses know that it’s a life support system and 71.4% know that it’s indicated for patients with respiratory failure, 81% of nurses perform chest physiotherapy to reduce the risk of pneumonia in ventilated patients .But the study found that less than half of the nurses (31%) Auscultate breathe sounds in order to assess ventilated patients. This indicates that they lack the assessment skills which can lead to patient sustaining more secretions and ultimately developing more complications.
Other specific objective of this study was regarding nurse assessment about the knowledge of the patient in need for endotracheal suctioning. This study revealed that 64.3% look for visible or audible secretion in their assessment) and only 47.6% said that wheezes are not an indication for suctioning after auscultation. 42.9% of nurses use ABG to monitor oxygenation . Difficulty to assess secretions presence makes secretions stagnate leading it to become thick and very difficult to suction.
Another objective was nurse’s knowledge regarding endotracheal suctioning. revealed that half of nurses 47.6%said it’s used to remove secretion form the artificial airway, while 38.1% of nurses said it’s used to remove secretion from the trachea itself which reflects nurse’s misunderstanding regarding the term (endotracheal), this leads to faulty procedure. The study also showed that 52.4% of nurses think that murmurs are not an indication for endotracheal suction .This result revealed that half nurses are unaware of the indication for suction making the patients prone to ventilator associated pneumonia and other complication.
Nurse’s knowledge regarding prevention of nosocomial infections is also assessed. Table 4-10 showed that only 47.6% of nurses wash hands and maintain aseptic technique to prevent nosocomial infection. This low percentage calls for more efforts to be put in this matter because patients will be in great danger of catching cross infections.
The study also assessed knowledge regarding suction catheter size. It revealed that over half the nurses 64.3% use a size that is less than the internal diameter of the tracheal tube, correct tube size decreases patient distress and tracheal mucosa damage.
Knowledge of preoxygenation, suctioning duration, interval and source pressure was also assessed. The study showed that 64.3% of nurse’s know that it minimizes hypoxia, 45.2% suction for 10-15 seconds, 45.2% uses 80-120 mmhg pressure, 61.9% suction only when clinically indicated. Correct suction interval and pressure reduces hypoxia and atelectasis.
Regarding complication and adverse effects of endotracheal suction, the study revealed that 45.2% of nurses think that decreased blood volume is not a complication, only 14.3% said that it causes reduction in lung volume, and only 14.3% think that patients with high intracranial pressure and severe hypertension both are contraindicated from the procedure. Nurses lack of knowledge regarding complications, adverse effects and contraindications complicates patient status even more.
Nurse’s knowledge pertaining normal saline instillation and its effect was also assessed. Table1-19 revealed that only 14.3% of nurses said that saline instillation during suction procedure it’s not recommended, 42.9% of nurses think that tachycardia, Dyspnea, ventilator associated pneumonia are the result of instilling saline during suction procedure this can only mean that the nurses are not updated to current practice guidelines regarding saline instillation.
The knowledge about the effect of increased frequency of suctioning was also assessed. Result showed that only 16.7% of nurses said that it causes atelectasis. This result reflects nurse’s lack of knowledge pertaining suctioning frequency. Suctioning the patient too much would damage the lung mucosa.
Nurse’s knowledge regarding discontinuation of the procedure was assessed. Result showed that only 14.3% think that changes in heart rate and cardiac ectopy both are predictors for stopping the procedure, on the other hand, majority of nurses 50% think that only changes in heart rate is a predictor for stopping the procedure while 31% reject both options. This study reflects that nurses don’t monitor patients during the procedure.
Pertaining adverse effects of hyperinflation, this study showed that only 14.3% of nurses think that low cardiac output is exception. This thing reflects poor knowledge regarding adverse effects of hyperinflation.
Total knowledge was assessed using grading scale for knowledge. (Figure.1) demonstrates total knowledge level in Khartoum teaching hospital and as observed the majority of ICU nurses 85.7% have poor knowledge. This can give a full picture of knowledge level and indicate that the majority of ICU nurses working in Khartoum teaching hospital lack knowledge regarding endotracheal suctioning procedures. This agrees with what Day found in her studies in 2001 for knowledge assessment for ICU nurses (7) and her 2002 study for knowledge assessment and relationship between practice and knowledge.
This knowledge could aid the nurses to facilitate early recovery of the patients, hasten discharge and enhances cost effectiveness through reduction of hospital stays (10).
The study also assessed the practical level of ICU nurses (Table 2), result showed that all nurses 100% check functioning of suctioning apparatus, monitor heart rate and record blood pressure but none of them 100% Auscultate breath sounds which indicate that they don’t assess the patient.
Over half of nurses 80% don’t wear face mask, and all of them 100% don’t use sterile gloves reflecting their negligence for infection control issues.
46.7% of nurses don’t pull back if resistance is met and don’t withdraw catheter while rotating back, 66.7% don’t limit suction time to 10-15 seconds, 53.3% suction more than 4 times reflecting the deficiency in performing suction procedure.
The majority of nurses 80% don’t assess patient’s cardiopulmonary status or secretion clearance after suctioning procedures. 100% don’t note changes in vital signs or document the procedure or wash and replace the articles. This reflects the nurse’s deficient in the aftercare actions for the procedure.
The total practice level was analyzed by practice grading scale. As observed in this study, figure.2 demonstrates that 76.6% of nurses have fair practice level. There is Significant discrepancies were observed in ICU nurses’ performance in relation to current recommendations in their practice prior to, during and post ETS actions. This matches what Celik and Elbas found in their research in Austria hospital ICU 2000 (6). Also matches what Miia found in her study in 2013 in Finland hospital ICUs that the ETS practices prior to, during and post events was significantly lower than the required quality of care (2).
Other discrepancy observed in this study that the practical level was significantly better than knowledge level. This opposes what Mary found in her 2005 study, as she found that nurse practical level was worse than knowledge level (7).
Normally; as working experience increases; knowledge and practice level also increase. There is no significant relationship between years of experience, knowledge and practice. P-value is (0.905, 0.962) for knowledge and practice level respectively. This matches what Mary found in her research in Indian hospitals 2005 (7).When the results were compared, both in practice and knowledge, with the years of experience in ICU, no statistically significant differences were found.
The present study conclude the majority of Khartoum teaching hospital nurses are working there for more than 3 years, but their knowledge and practice level of ETS wasn’t affected by their length working experience.
Nurses working in Khartoum teaching hospital have fair practical level regarding their action prior to, during and after the ETS procedure, but this study shed light to the fact that even though their practice was fair, it is clearly better than their knowledge. This can be manifested by the lack of good supervision and guidance.
The present study conclude the Khartoum teaching hospital nurses have poor knowledge concerning mechanically ventilated patient’s assessment, Assessment for the need of endotracheal suction and Basic information about endotracheal suctioning procedure.
The present study recommended that is need for Practice guidelines and teaching programme to be implemented and updated monthly or annually in all hospitals.
References
- Guglielminotti J, Desmonts J, Dureuil B. Effects of tracheal suctioningon respiratory resistances in mechanically ventilated patients. Chest 1998; 113(5):1335-1338.
- Miia J, Tero A, Pekka Y, Helvi k. Evaluation of endotracheal-suctioning practices of critical-care nursesJournal of Nursing Education and Practice,January2013.
- Mohammad A, Alireza I, Atye B, Mehdi S, Jahanbakhsh V. Comparison the Effects of Shallow and Deep Endotracheal Tube Suctioningon Respiratory Rate, Arterial Blood Oxygen Saturation and Number of Suctioning in Patients Hospitalized in the Intensive Care Unit. Journal of Caring Sciences, 2014, 3(3), 157-164
- Wood CJ.endotracheal suctioning: a literature review. Intensive Crit Care Nurs. Jun 2004; 14(3):124-36.
- Carsten M. Pedersen. Mette R. Jeanette H. Ingrid E. endotracheal suctioning of the adult intubated patients. Intensive and critical care nursing 2009: 25, 21-30.
- Tharnamme, pneumonia in mechanically ventilated patient’s journal of medical association 2000; 56(2):102-4.
- Mary P. effectiveness of endotracheal suctioning technique. Nursing journal of India, may2005; 28(6):5-7
- Day T.L., Wainwright S. & Wilson-Barnett J. An evaluation of a teaching intervention to improve the practice of endotracheal suctioning in post cardiac patients in intensive care units. Journal of Clinical Nursing 2001; 10, 682–696.
- Tablan OC, Anderson LJ, Arden NH, Breiman RF, Butler JC, McNeil MM. (2006).Guideline for prevention of nosocomial pneumonia. The Hospital Infection 13. Control Practices Advisory Committee, Centers for Disease Control and Prevention. Am J Infect Control; 22:247-92.13
- Intensive care coordination and monitoring unit ICCMU. Health Statewide Guidelines for Intensive Care: Suctioning an Adult with a Tracheal Tube-2007 revision & update. Retrieved 2010:1iccmu@wahs.nsw.gov.au.
- American Association for Respiratory Care (AARC). Clinical Practice Guidelines. Endotracheal suctioning of mechanically ventilated patients with artificial airways. Respiratory Care. 2010; 55: 758-64. PMid: 20507660.



