
International Journal of Preventive Medicine Research, Vol. 2, No. 4, August 2016 Publish Date: Nov. 2, 2016 Pages: 17-22
The Effect of Health Educational Program on Patients' Knowledge About Hypertension and Its' Management (In Sudan - White Nile State)
Ahmed Abdalla Ahmed Jarelnape1, *, Nader T. Mohammed Abdullah2, Kalthoum Ibrahim Yousif3, El-Saida Abdel Mageed El-Rufai3
1Medical-Surgical Nursing, Faculty of Nursing, Al-Ghad International College, the National Ribat University, Khartoum, Sudan
2Applied Medical Sciences, Al-Ghad International College, Jeddah, Kingdom of Saudi Arabia
3Faculty of Nursing Sciences, the National Ribat University, Khartoum, Sudan
Abstract
Background: The incidence of hypertension (HTN) has increased rapidly in the Sudan in the last few years Objective: The present study aimed to examine the hypertensive patient knowledge who receive health education program about hypertension and its management. Methods: This Quasi-experimental study was conducted on 150 patients with hypertension attending outpatient clinics of the two health centres. Demographic and clinical data including the compliance different aspects of hypertension disease including definition, types, risk factors, symptoms, complications, main aspects of self-care, and main aspects of dietary management and importance of physical activity for hypertension patients were collected. The data were collected from all patients and the analysed using SPSS version 19 software, and independent t-test was used for significance tests at 0.05 level. Results: Results of the current study, regarding correct knowledge of the studied group before and after the health education program and the different aspects of hypertension, showed that there was a significant improvement of the patients' knowledge concerning the correct knowledge of the definition of hypertension, signs and symptoms of hyper and hypotension, compliance to drug types of treatment dietary management, importance of exercise and complications of hypertension, (P < 0.001). Conclusion: The study showed that patients with hypertension in Sudan have low knowledge about hypertension and his managements. Patient education, and public enlightenment are imperative
Keywords
Hypertension, Knowledge, Management, Sudan
Received: October 14, 2016
Accepted: October 26, 2016
Published online: November 2, 2016
@ 2016 The Authors. Published by American Institute of Science. This Open Access article is under the CC BY license. http://creativecommons.org/licenses/by/4.0/
Contents
1. Introduction
Hypertension (HTN) is universally accepted as one of the most important risk factors in the development of cardiovascular disease (CVD), stroke and renal disease [1, 2]. There has been a considerable increase in the prevalence of HTN in the Middle East during the last few years. In some Arab countries hypertension has become a major health problem [3]. This drastic increase in incidence of hypertension is specifically caused by a combination of many parameters, including family history [4]. Change in lifestyle, dietary habits and environmental factors [5]. Sudan is considered one of the leading countries in Africa for the prevalence of hypertension [6] However, a proper national registry on hypertension is not available in Sudan and evaluation studies are rarely done [7]. Nevertheless, a recent study showed an increasing incidence of hypertension in Sudan [8]. Which may result in serious health problems in the near future if no appropriate measures are taken. The prevalence of hypertension may be a result of the marked shift in the Sudanese diet, which has resulted in increased overweight and obesity [3]. Some studies have claimed the prevalence of hypertension is a cause of the tremendous increase in renal insufficiency [2]. Increased awareness, follow up and control of hypertension in industrialized countries has resulted in a decreased tendency to morbidity and mortality from cardiovascular disease [9]. To reach the level of improvement attained in developed countries, epidemiological studies on the risk factors, control methods, control levels, lifestyle, adherence to medication, and awareness will be crucial for setting control strategies in Sudan. In this study was examine the hypertensive patient knowledge who receive health education program about hypertension and its management
2. Materials and Methods
This A quasi-experimental study was conducted on patients with hypertension This study was carried out in two health centres at White Nile state Kosti city. A total of 150 Sudanese HNT patients were randomly selected from two health centres, On February, 2013. The patients participated registered hypertension patients Age 30 years and above, both sex’s male and female, diagnosed with hypertension, able to communicate, visiting the clinic regularly for treatment or follow up. (Monthly or Biannually).
The questionnaire consists of 40 multiple choice questions covering different aspects of hypertension disease including definition, types, risk factors, symptoms, complications, main aspects of self-care, and main aspects of dietary management and importance of physical activity for hypertension patients.
Revised hypertension knowledge Questionnaire was used, on a 4 levels: those who correctly answered less than 15 to 25 hypertension knowledge questions were considered to have poor knowledge, those who answered 25 to 50 of questions as having moderate knowledge, those who answered 51 to 75 of questions as having good knowledge and those who answered more than 76 as having Very good knowledge [10].
The basic information questionnaire was developed with informed consent and validated by nurse educator and then tested on 10 patients. The questionnaire was filled by the researcher through using a clear Arabic language, the questionnaire includes the following sections: Patients file number, place of residence and telephone number, Socio-demographic data: including sex, age, marital status educational level, income level, Anthropometric measurements: including height, weight, body mass index, blood pressure, Hypertension related data: Duration of disease, family history of hypertension, other treatment, and presence of complications, Health Education data: Previous health education programs and Lifestyle data: including smoking, daily and previous physical activity and dietary history.
Data was presented using descriptive statistics including frequency, percentage, mean with standard deviation (SD) and P-value of ≤0.05 was considered statistically significant for relationship investigations. Ethical clearance was obtained from the local Ethics Committees at the National Ribat University, All patients gave their written informed consent to participate in the study.
3. Results
Table 1. The study showed on 45 (60%) were males and 30 (40%) were females on control group is likely same above value 43 (57%) were males and 32 (42%) were females, (40%) were 40 years old. The mean ± standard deviation of age was 2.15 ± 0.77 for intervention group and 2.01 ± 0.78 for control group. The majority of subjects (72%) were married in intervention group and (73%) for control group. Most of subjects (73%) were working in intervention group and (70%) on control group. There is no significant difference between intervention group and control group on the demographic characteristics at the level of (P 0.05).
Table 1. The socio-demographic variables of the study population (n=75) in Sudan.
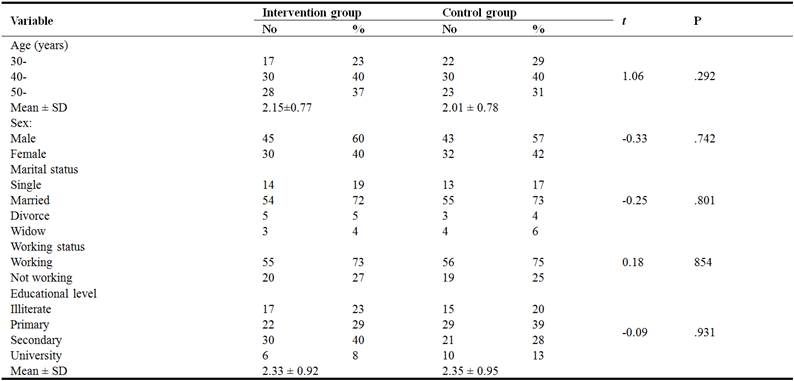
Table 2. Shows The result of the mean value of patient's knowledge regarding definition of hypertension before attending of educational programs was 0.41±0.50 while the mean knowledge of the patients after the program on the same dimension was 0.87±0.34, There is a significant difference (P = 0.001 < 0.05). The mean value of patient's knowledge regarding causes of hypertension before attending of educational program was 0.25±0.44 while the mean knowledge of the patients after the program on the same dimension was 0.92±0.27, there is a significant difference (P = 0.002 < 0.05). The mean value of patient's knowledge regarding signs & symptoms of hypertension before attending of educational program was 0.32±0.47 while the mean knowledge of the patients after the program on the same dimension was 0.93±0.25, there is a significant difference (P = 0.003 < 0.05). The mean value of patient's knowledge regarding signs & symptoms of hypotension before attending of educational program was 0.40±0.49 while the mean knowledge of the patients after the program on the same dimension was 0.88±0.33, there is a significant difference (P = 0.007 < 0.05). The result of The mean value of patient's knowledge regarding Importance of compliance to types of drugs about hypertension before attending of educational program was 0.32±0.47 while the mean knowledge of the patients after the program on the same dimension was 0.55±0.50, there is a significant difference (P = 0.005 < 0.05). The mean value of patient's knowledge regarding Importance of compliance to medication regimen about hypertension before attending of educational program (n=75) was 0.12±0.33 while the mean knowledge of the patients after the program on the same dimension was 0.65±0.48, there is a significant difference (P = 0.004 < 0.05). The mean value of patient's knowledge regarding Importance of compliance to dietary program about hypertension before attending of educational program was 0.23±0.42 while the mean knowledge of the patients after the program on the same dimension was 0.73±0.45, there is a significant difference (P = 0.004 < 0.05). The mean value of patient's knowledge regarding Importance of compliance to exercise about hypertension before attending of educational program was 0.32±0.47 while the mean knowledge of the patients after the program on the same dimension was 0.80±0.40, there is a significant difference (P = 0.004 < 0.05).
Table 2. Distribution of correct knowledge about hypertension disease aspects (N=75).
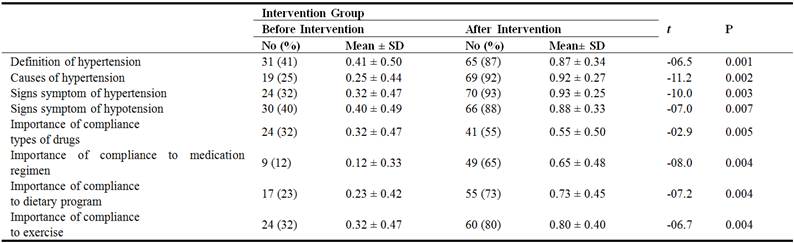
Table 3. Shows the result of the mean value of patient's correct knowledge regarding vascular complications of hypertension before attending of educational programs was 1.88±0.33 while the mean knowledge of the patients after the program on the same dimension was 1.37±0.49, there is a significant difference (P < 0.05). The mean value of patient's correct knowledge regarding renal complications of hypertension before attending of educational programs was 1.83±0.38 while the mean knowledge of the patients after the program on the same dimension was 1.33±0.47, there is a significant difference (P < 0.05). The mean value of patient's correct knowledge regarding eye complications of hypertension before attending of educational programs was 1.85±0.36 while the mean knowledge of the patients after the program on the same dimension was 1.21±0.41, there is a significant difference (P < 0.05). The mean value of patient's correct knowledge regarding cardiac complications of hypertension before attending of educational programs was 1.81±0.39 while the mean knowledge of the patients after the program on the same dimension was 1.20±0.40, there is a significant difference (P < 0.05).
Table 3. Distribution of correct knowledge about hypertension complications (n=75).

Table 4. Shows the result of the mean value of patient's correct knowledge about change the diet program for hypertension disease before attending of educational programs was 1.88 ± 0.33 while the mean knowledge of the patients after the program on the same dimension was 1.33± 0.47, there is a significant difference (P = 0.000 < 0.05). The result of the mean value of patient's correct knowledge about maintaining healthy dietary habits for hypertension disease before attending of educational programs was 1.92±0.27 while the mean knowledge of the patients after the program on the same dimension was 1.09±0.29. There is a significant difference (P = 0.000 < 0.05).
Table 4. Distribution of correct knowledge about hypertension dietary program (n=75).

Table 5. Show The most common source of knowledge related to information about hypertension for the patients in (Intervention group) was found to be Friends/Relatives (41.3%) followed by Mass media: Television/Newspaper (30.7%). In only 21.3% cases the knowledge was obtained from medical and paramedical professionals. And (6.7) from others sources, the percentage is similar for the control group. There is no significant difference (p > 0.05).
Table 5. Distribution of Sources of information knowledge regard hypertension disease.

4. Discussion
Regarding concerning correct knowledge of the intervention group in table 2 about definition of hypertension signs & symptoms, causes and etc…., results of the study showed more half of the hypertensive patients 68.0% had average or poor knowledge about hypertension, whereas only 16.0% patients had very good knowledge about the hypertension on the same dimension. It was improve after educational intervention to (73.3). This finding is supported by Williams MV et al [11]. In their study in 402 hypertensive patients, also found 189 patients (47.02%) did not have adequate knowledge about hypertension. Similar inadequacy of knowledge, awareness and practice of hypertension among Indian patients has been reported by (Hemant Mahajan) [12]. Importance of compliance to (drugs, medication regimen, dietary program and exercise) it was improve after educational intervention. However, the scours of knowledge was significantly increased after the educational intervention, demonstrating the beneficial effects of education on the patient’s knowledge. This result supported by (Falaschetti E, et al) He said hypertension control signifies a greater need to increase the awareness of hypertension related information among the patients [13]. The possible reasons to lower knowledge may be because of lower literacy, inappropriate perception of medical advice, irregular sources of health related information, or inadequate counselling regarding hypertension possibly due to skewed doctor patient ratio in government run hospitals [14]. Regarding sources of knowledge for hypertension the patients reported to have derived their knowledge about Hypertension majorly from non-medical sources like friends/relatives and mass media communications. (72%) and only (21.3%) of sources were from medical professionals like doctors, specialist paramedical staff, which form the more reliable source to provide health related information. Therefore the patient has to be alerted to scrutinize the information received, from their doctors and work in collaboration with health providers to get valid information. The knowledge from such unreliable sources may be the cause of lower awareness among the population. Considering the influence of mass media on the population, a possible alternative to increase awareness may be by means of delivery of such information using mass media. This findings supported by (Hroscikoki MC, et al) [14]. Reported that positive role of pharmacist mediated counselling of hypertensive patients, regarding risk factor and associated co-morbidities, while some other studies suggest that knowledge transferred from medical staff is an important factor in inducing patient to comply with lifestyle modification [14]. Nevertheless; low counselling rates were reported in similar studies [15, 16]. About knowledge about lifestyle modifications (change the diet program and maintaining continuous follow up) study showed most of hypertensive patients knowledge about lifestyle modifications (32.0%) before education program, It was improve after educational intervention to (74.7). These result supported by many authors (Chiu CW, Ostovan MA) They said Patient’s involvement in self-monitoring and management, together with continuous follow up has also been recommended by others [17, 18]. Similarly, Wang YR et al. emphasized that the most important points for BP control were lifestyle modifications, home BP monitoring, reinforcement of healthy behaviours, and continuous follow up [19]. In (Aubert et al) study, most patients believed that salty diet, obesity and smoking are important factors in hypertension. They mentioned that physical activity and exercise are very important factor in hypertension management [20]. Regarding hypertension complications the study showed patient's knowledge (15%) before attending of educational programs it was improve after educational intervention to (75%). These findings were supported by previous study results shown a positive relationship between patients' knowledge about the hypertensive complications and adherence [21]. In addition, they are aware of hypertension complications and advantages of lowering blood pressure Most cases agreed that decreasing blood pressure (even a little bit) could be effective on health and decrease there complications [22].
The strengths of this study include the study conducted in developing countries with limited resources. The study limitations were; the study was conducted as a descriptive study; interventional studies will yield more useful results if conducted on more sample with complete randomization all over the country.
5. Conclusion
After the analysis of the study variables the researcher justify the findings and conclude that: The results from this short educational intervention program on hypertensive patients in health clinic in Kosti City indicated that knowledge changes in a positive results in all the variables related to patients knowledge. In the current study, the majority of the patients did not have sufficient knowledge to complications of hypertension at the pre-test phase, education program effect and improve their knowledge about complication post-test there is a significant difference (P < 0.05).
Also in the current study, the majority of the patients get information about hypertension and its management from non-medical sources (from friends/Relatives (41.3%) followed by mass media: Television/Newspaper (30.7%). In only 21.3% cases the knowledge was obtained from medical and paramedical professionals. In the current study, the most of the patients did not have controlled blood pressure at the pre-test phase only 32% of patients controlled blood pressure, Post-test after intervention 92% of patients controlled blood pressure and good knowledge to adjust their blood pressure lifestyle changes involving dietary and exercise being effective in significant decrease in weight, and effective in improving patient’s knowledge.
Recommendations
After obtaining the study findings based on the conclusion, the researcher recommended that: The educational intervention program should be developed in hypertension clinics in primary health care centres in Sudan. Since primary health care providers have a better chance to meet with patients, promotion of hypertension educational intervention programs by these centres will increase the effectiveness of hypertensive therapy and will delay the onset or the progression of complications, improve the quality of life for hypertensive patients and reduce the associated medical costs. Educating the patient’s family about hypertension disease meal planning and their dietary management and the relationship between obesity and the chance of disease occurrence. Educating the family about the importance of involvement of hypertensive patient s food with family food. The ideal treatment would consist of a comprehensive and multidisciplinary Hypertension disease team. (Physician, Nurse, Nutritionist, Pharmacist, Social worker, foot specialist and others). Training of the hypertensive care team on the management of hypertension and how to educate the hypertensive patients Establishment of regional records for hypertensive patients in order to facilitate health care and health education for them.
References
- Ruilope LM, Schiffrin EL. Blood pressure control and benefits of antihypertensive therapy: does it make a difference which agents we use? Hypertension. 2001; 38 (3 Pt. 2): 537–542.
- Whelton PK, Perneger TV, Brancati FL, Klag MJ. Epidemiology and prevention of blood pressure-related renal disease. J Hypertension Suppl. 1992; 10 (7): S77–84.
- Musaiger AO. Diet and prevention of coronary heart disease in the Arab Middle East countries. Med Princ Pract. 2002; 11 (Suppl 2): 9–16.
- Shehata MF. A proposed study on how far anger contributes to initiating essential hypertension in Canadian Caucasian adults with family history of hypertension. Clin Med Insights Cardiology. 2010; 4: 9–13.
- Ghannem H, Fredj AH. Epidemiological transition and cardiovascular risk factors in Tunisia. Rev Epidemiology Sante Publique. 1997; 45 (4): 286–292.
- Tesfaye F, Byass P, Wall S. Population based prevalence of high blood pressure among adults in Addis Ababa: uncovering a silent epidemic. BMC Cardiovascular Disorder. 2009; 9: 39.
- Abu-Aisha H, Elhassan EA, Khamis AH. et al. Rates and causes of peritonitis in a National multicenter continuous ambulatory peritoneal dialysis program in Sudan: first-year experience. Saudi J Kidney Disease Transplant. 2007; 18 (4): 565–570.
- Ahmed ME. Blood pressure in a multiracial urban Sudanese community. J Hum Hypertens. 1990; 4 (6): 621–624.
- Wolf-Maier K, Cooper RS, Banegas JR. et al. Hypertension prevalence and blood pressure levels in 6 European countries, Canada, and the United States. J Am Med Assoc. 2003; 289 (18): 2363–2369.
- Saleem F, Hassali MA, Shafie AA, Awad AG, Bashir S. Association between knowledge and drug adherence in patients with hypertension in Quetta, Pakistan. Tropical Journal of Pharmaceutical Research. April 2011; 10 (2): 125-132.
- Williams MV, Baker DW. Relationship of functional health literacy to patient’s knowledge of their chronic disease. A study of patients with hypertension and diabetes. Arch Intern Med, 1998 Jan 26; 158 (2): 166-72.
- Mahajan H, Kazi Y, Sharma B, Velhal GD. Assessment of KAP, Risk Factors and Associated Co-Morbidities in Hypertensive Patients, (Sep-Oct. 2012), PP 06-14.
- Falaschetti E, Chaudhury M, et al. Continued improvement in hypertension management in England: results from the Health Survey for England 2006. Hypertension. 2009 Mar; 53 (3): 480-6.
- Hroscikoki MC, Solberg LI, et al: Challenges of change a qualitative study of chronic care model implementation. Ann. Fam. Med. 2006 Jul-Aug; 4 (4): 317-26.
- Prochaska J. DiClemente C. The Trans theoretical Approach: Crossing traditional boundaries of therapy. Homewood II: Dow Jones-Irwin, (1984).
- Stange KC, Flocke SA, et al. Direct observation of rates of preventive service delivery in community family practice Preventive.2000 Aug; 31 (2 Pt 1): 167-76.
- Chiu CW, Wong FK. Effects of 8 weeks sustained follow-up after a nurse consultation on hypertension: a randomized trial. International journal of nursing studies. [Randomized Controlled Trial Research Support, 2010.
- Ostovan MA, Zibaeenezhad MJ, et al The impact of education on weight loss in overweight and obese adults. International cardiovascular research journal. 2013 Sep; 7 (3): 79–82.
- Wang YR, Alexander GC, Stafford RS. Outpatient hypertension treatment, treatment intensification, and control in Western Europe and the United States.2007 Jan; 167 (2): 141-7.
- Aubert L,Bovet P,Gervasoni JP,Rwebogora A,Waeber B,et al.Knowledge, attitudes, and practices on hypertension in a country in epidemiological transition. 1998 May; 31 (5): 1136-45.
- Ghembaza MA,Senoussaoui Y,Tani MK,Meguenni K. Impact of patient knowledge of hypertension complications on adherence to antihypertensive therapy. 2014; 10 (1): 41-8.
- Egan BM,Lackl and DT,Cutler NE. Awareness, knowledge, and attitudes of older Americans about high blood pressure: implications for health care policy, education, and research. 2003 Mar 24; 163 (6): 681-7.



