
International Journal of Preventive Medicine Research, Vol. 1, No. 3, August 2015 Publish Date: Jul. 11, 2015 Pages: 153-160
A Study of Overweight and Obesity Among Secondary School Students in Dubai: Prevalence and Associated Factors
Hamid Y. Hussain*, Al Attar F., Makhlouf M., Ahmed A., Jaffar M., Dafalla E., Mahdy N., Wasfy A.
Department of Health and Medical Services, Primary Health Care, Public Health Affaires Section, Dubai, UAE
Abstract
Obesity is a major public health problem all over the world. It has become a global epidemic in both industrialized and developing countries. The dramatic increase in the prevalence of obesity among school children is associated with significant health and financial burdens; warranting strong and comprehensive prevention efforts. Objectives: Measurement of the prevalence of overweight and obesity among secondary school students in Dubai and determination of the associated factors. Materials & methods: Multistage stratified random sample was carried out in secondary schools in Dubai. The stratification was based upon region, gender and language. One class from each grade of educational level was selected randomly. The students were subjected to a self-administrated questionnaire that included personal data, family history, and dietary habits. Weight and height were measured. The sample amounted to 1186 students. Results: The results revealed that the prevalence of overweight and obesity was 26.7%, 12.2% respectively. Male encountered a significant higher percentage of overweight & obesity (30.1% &15.4% respectively) than females (23.1% & 8.9% respectively, p<0.05). Non- national students experienced a higher percentage of overweight & obesity (29.2% & 12.8% respectively) compared to nationals (20.2% &10.6% respectively) and this was statistically significant. It was found that students in grade ten were more likely to become overweight or obese compared to those in grades eleven or twelve(30.8%, 25.2 % & 22.1% for overweight respectively) and for obesity (15.3%, 10.4% & 9.7% respectively). Stepwise logistic regression analysis delineated five predictors for overweight and obesity. These predictors were in order: eating fast food regularly, positive family history of obesity, male gender, those in tenth grade and non- national students; the associated risks were (OR = 1.44, 1.51, 1.79, 1.72, and 1.41 respectively). Conclusion & recommendations: The present study revealed that overweight and obesity are highly prevalent among secondary school students in Dubai. Urgent and effective community intervention programs are highly required in order to combat this problem.
Keywords
Overweight, Secondary Schools, Dubai
Received:May 11, 2015
Accepted: May 21, 2015
Published online: July 8, 2015
@ 2015 The Authors. Published by American Institute of Science. This Open Access article is under the CC BY-NC license. http://creativecommons.org/licenses/by-nc/4.0/
1. Introduction
Obesity is a major public health problem all over the world. It has become a global epidemic, and it is still increasing in both industrialized and developing countries. The alarming increase in the prevalence of obesity over the last few decades has raised concerns about associated health risks for children, adolescents as well as adults.(1)
Obesity is one of the greatest public health challenges of the 21st century. Its prevalence has tripled in many countries since the 1980s, and the numbers of those affected continue to rise at an alarming rate, particularly among children and adolescents.(2) The most comprehensive data on the prevalence of obesity worldwide are those of the World Health Organisation MONICA project (Monitoring of trends and determinants in Cardiovascular diseases study).(3) Together with information from national surveys, the data show that the prevalence of obesity in most European countries has increased by about 10-40% in the past 10 years, ranging from 10-20% in men and 10-25% in women. (4) The growing prevalence of obesity among children is also a major concern (data from 79 developing countries and a number of industrialized countries suggests that about 22 million children under 5 years old are overweight world-wide. (5)
Between 1995 and 2002, obesity doubled among boys in England from 2.9% of the population to 5.7%, and amongst girls increased from 4.9% to 7.8%.(6). In USA, Obesity prevalence in youths aged 12-17 has increased dramatically from 5% to 13% in boys and from 5% to 9% in girls between 1966-70 and 1988-91. (2)
Similar data now are being reported from many developing countries, particularly in those in Asia and, to a lesser extent, in Africa. In Bahrain(7), studies showed a marked increase in obesity noted more among adolescents, ranging from 15% to 45%. In United Arab Emirates (UAE), A national study (8)wasdone to assess the prevalence of obesity among school children, revealed that UAE children are at increased risk for overweight and obesity. Obesity was 2.3 folds higher among UAE boys and girls at 14 years compared to international standards and reached to 3.6 and 1.9 folds higher among UAE boys and girls respectively at the age of 18 years.
Obesity is associated with significant morbidity and mortality, including coronary heart disease, hypertension, type 2 diabetes, respiratory (obstructive sleep apnea), orthopedic, gastrointestinal, endocrine, musculoskeletaldisorders, selected cancers, social and psychosocial morbidities, as well as the economicimpact of obesity (9). Obesity is the cause of 300,000 deaths each year. Childhood obesity seriously increases the risks of acquiring obesity-related medical conditions later in life (10). It was also found that obese children and adolescents reported significant impairment in physical, psychosocial, emotional, and school functioning, which was 5.5 times greater than that for healthy children or adolescents (11).
Obesity is a complex, multifactoral and chronic condition resulting from interplay between genetics and environment (1). Genetics influence how the body regulates appetite and metabolism, while certain environmental factors encourage excess calorie consumption (12).
Worldwide, the adoption of industrialized western society lifestyles (an increase in consumption of fats, oils and refined carbohydrates and a decreased intake of complex carbohydrates together with increased sedentariness and car ownership) is associated with increasing obesity. Changes in meal patterns and leisure time are also implicated (13).
The importance of the study come from the dramatic increase in the prevalence of obesity among school children is warranting strong and comprehensive prevention efforts. Schools have been identified as a key setting for public healthstrategies to prevent overweight and obesity. (14)
2. Aims of the Work
The present study aimed to measure the prevalence of overweight and obesity among secondary school students in Dubai and to determine the associated factors.
3. Subjects & Methods
3.1. Study Setting and Design
A cross sectional study was carried out in private schools in Dubai, data collection started February 2010 and completed on April 2011.
3.2. Target Population
Secondary school students .
3.3. Sampling Design
A- Sample size
Using the computer program EPI_INFO "6.04", prevalence of obesity 13.5%(27), 2% degree of precision and 95% confidence limits, the minimum sample size required is 1121 students.
B- Sampling technique
A Multistage stratified random sample with equal allocations was carried out. The stratification was based upon region (Bur Dubai, Deria), gender (males, females) and language in schools (Arabic & non Arabic). One class from each grade of education was selected randomly and all the students was invited to participate in the study, the sample amounted to 1186 students.
N.B The weight and height was not measured for 53 students, the sample size was 1133.
3.4. Data Collection Plan
All students were subjected to a self administrated questionnaire and anthropometric measurements. The following data were data included:
• Sociodemographic characteristics such as age, sex, nationality, parent's education.
• Family history of obesity.
• Dietary habits: Dietary history including 6 questions about the frequency of taking breakfast, fruits &vegetables ,soft drink ,snakes &nuts ,sweets and fast food. The answers of the questions were divided into: Regular: one or more intake /day. Irregular: < 3 intake /week.
• Life style: physical activity(>3 times /week), playing computer games or watching TV (<2 hours and 2 hours or more).
• Anthropometric measurements: weight & height.
• Body mass index (BMI) was calculated for each student using the formula: BMI = Weight (Kg)/ Height (m2).
Table (1). The Body mass index (BMI) classified by percentiles according to (CDC, 2000). (15)
| Underweight | Less than the 5th percentile |
| Healthy weight | 5th percentile to less than the 85th percentile |
| overweight | 85th to less than the 95th percentile |
| Obesity | Equal to or greater than the 95th percentile |
3.5. Statistical Analysis
The statistical analysis was carried out using computer program SPSS version "12". The following statistical analyses were performed:
• Chi-square test (16): was used for categorical data. To examine the relationship between sociodemographic, dietary habits and life styles and overweight and obesity.
• Stepwise logistic regression (17): was used to delineate the predictors for overweight and obesity.
• P<0.05 was used as cut off level of significance.
N.B All cross tabulation tables with Chi-square test were conducted using the four categories of BMI percentile classification (underweight, healthy weight, overweight & obese) and the data related to overweight and obesity were only presented.
4. Results
The present study comprised 1186 secondary school students, their mean age was 15.76 ± 0.93 years. More than one half was male students (50.6%). Non-nationals constituted 70.5% of the students. University or higher level of education was detected for almost half of the student's mothers, and for 70.5% of the students' fathers. Family history of obesity was reported among 31 % of the students.
Figure (1) presents the distribution of the students according to body mass index percentile, it displayed that 115 (10.1%) were underweight, 578 (51.0%) were within healthy weight, 302 (26.7%) of students were overweight and 138 (12.2%) were obese .
From table (2) it can be observed that there was a significantly higher percentage of overweight and obesity among males compared to females (30.1% versus 23.1% respectively for overweight) and (15.4% versus 8.9% respectively for obesity, X32 = 23.62, p<0.05).
Non-national students experienced a higher significant percentage of overweight and obesity compared to nationals (29.2% versus 20.2% respectively for overweight) and (12.8% versus 10.6% respectively for obesity), X32 = 15.35, p<0.05.
It was found that students in grade ten were more likely to be overweight and obese compared to those in grades eleven or twelve (30.8%, 25.2% & 22.1% for grade 10, 11 and 11 respectively) and obesity (15.3%, 10.4% & 9.7% respectively) and the difference was statistically significant (X62 = 19.24, p<0.05).
As regards the family history of obesity , the table clarified that students with positive family history demonstrated a higher percentage for overweight and obesity (30.2% & 14.2% respectively) compared to those without such history (25.1% & 11.3% respectively, X32 = 10.20, p<0.05).
As regards the relationship between mother’s education and obesity, the table revealed that the lowest percentage of overweight and obesity was observed among students with mothers of high educational level (24.7% & 10.8% respectively) compared to those with non-educated (26.1% & 11.1% respectively)or those with moderate educational level (30.8% & 15.6% respectively), but this difference was not statistically significant.
Concerning the dietary habits, it was found that reported regular eating of snacks& nuts, sweet, fast foods was found in (48.7%, 44.6 %, and 36% of the students respectively and for soft drink (48.1%). As regards the life style, 43.6% were not practicing physical activity.
Table (3) presents the relationship between dietary habits, life style and BMI percentile of the student's. It was found that there was no significant association between regularity of eating breakfast, fruits & vegetables, or sweets and overweight or obesity. In addition, obesity was significantly higher among those with irregular eating of snakes than those with regular eating (13.3% versus 11%,P<0.05). On the other hand, the table revealed that 41.3% of those reported regular soft drink were overweight or obese compared to 36.6% among those with irregular drink (X32 = 11.44, p<0.05).
The table also yielded that those who reported eating regular fast foods were overweight and obese (30.8% & 13.9% respectively) compared to those reported irregular eating (24.4% & 11.2% respectively), X32 = 9.01, p<0.05.
As regards the physical activity practice, the table revealed that those who were practicing physical activity >3 times/week demonstrated a lower percentage of overweight and obesity (24.3% & 11.9% respectively) compared to those who were not practicing (29.7% &12.5% respectively),but this difference was not statistically significant. Furthermore, there was no significant association between hours of playing games or watching TV and overweight or obesity.
After adjustment of the confounders, the stepwise logistic regression (table (4)) delineated five predictors for overweight and obesity, the first predictor was eating fast food regularly, it was associated with risk of 1.44 relative to those who were eating it irregularly, the second predictor was family history of obesity as it was associated with the risk of 1.51 times of being obese relative to those without such history. The other predictors were in order; male gender, those in tenth grade and non-national students, the associated risks (OR) were (1.79, 1.72, and 1.41 respectively). Model X62 = 62.68, P<0.05.
Study limitations the cross sectional design will not let us know the causal relationship between obesity & overweight with risk factors. It only reflects the association relationship.
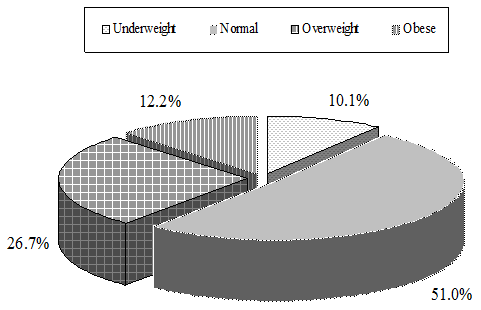
Figure (1). Distribution of secondary school students in Dubai according to BMI percentile.
5. Discussion
Overweight and obesity, as a feature of epidemiological transition, have long been recognized as a public health problem in industrialized countries. Recent evidence suggests that a similar phenomenon is emerging with the same velocity in most developing countries. (18) In Chesterfield County, USA, (19) it was found thatfrom 28 to 38% of children and adolescents were in high risk group; with a body mass index (BMI) between the 85th and 95th percentile (at risk for overweight) and > or = 95th percentile (overweight). In Italy (20), 8.4% of secondary school children were considered obese and 21.4% were considered at risk of overweight This increase in the prevalence of obesity is mostly due to life style changes (physical activity, leisure and modernization) and nutrition transition which are in relation with changing economic, social and health factors. (21) The Arabian Gulf countries moved toward the higher fat and higher refined carbohydrates western diet and this leads to obvious increase in the prevalence of obesity.(22) In Saudi Arabia, El Hazmi and Warsy 2002 (23) noted that the overall prevalence of overweight and obesity among girls aged 1-18 years was 12.7% and 6.7% respectively. Another study included female school-aged children and adolescents in primary and intermediate schools in Al-Khobar city, Kingdom of Saudi Arabia (24) revealed that the prevalence of overweight and obesity were 20% and 11%, respectively. In a study done in Bahrain secondary school students (25), it was found that 15.6% of boys and 17.4% of girls were either overweight or obese. In UAE, Malik and Bakir (2007)(26) conducted a study to determine the prevalence of overweight and obesity in children 5–17 years. The study revealed that 21.5% of children were overweight and 13.7% of them were obese.
The present study revealed higher percentage of overweight students and a closer figure for obesity to the previous study, where 26.7% of students were overweight and 12.2% were obese. Lower levels of obesity were detected among school children in UAE 2000 (8%) (27), in Al-Ain, 2000(10.4%) (28) and among primary female school children in Al-Ain City, UAE(2005) (8); where 11.1% and 15.8% were at risk of overweight or overweight. The higher rate of obesity in the present study and the study of Malik and Bakir (26), both conducted at 2007, may demonstrate the global trend of increase of obesity among school children. It may be also partly due to difference in gender representation in the other studies and the higher age of students in the present study as it includes only secondary school children. Increasing age of school children was associated with increased prevalence of overweight and obesity in different studies. (29, 30) kassmini etal 1997(31) found that overweight and obesity were more common among school children around the period of puberty. In another study (32), the prevalence of obesity decreased significantly with age, from 18.5% at 9 years to 7.6% at 14 years, rising at 15 years to 12.1%. During puberty, nutritional needs are increased due to physical growth, hormonal changes and emotional strain. At this adolescent age, they start eating out and take snacks in between meals. This may be due to increase requirement or may be the way of socializing. The snacks they eat are full of fats, carbohydrates and sugar. Some of them try to use food as a way to establish their identity, perhaps by over eating or going on a crash diet. (33)
The present study also revealed that children at grade 10 were significantly more overweight and obese than those in 11thor 12 thgrade. Grade 10 students are usually aged 15 to 16 years; which is usually the age following puberty. Older children may become more health oriented and caring for their body shapes before entry to the university, so they may do efforts to decrease their weight.
The present study also revealed that overweight and obesity are significantly higher among boys than girls. This goes with the national study,(27)which revealed that at age 18, UAE female obesity was one half the rate of obesity among UAE males. This was also found in different parts of the world. (20, 31) On the other hand, some studies(25, 26, 34) revealed higher prevalence of obesity among girls than boys. This controversy could be due different age of the included samples or different methods of assessing obesity. It could be also due to different cultural, environmental and ethnic factors. Differences in the prevalence of obesity due to ethnic factors were also found in different studies. (31, 35) The present study also showed that obesity is more common among non-national students compared to nationals. This was also previously found in UAE; (26) where non-national girls were more likely to be obese than UAE girls. Although ethnic factor may be important, other factors may be related as cultural, environmental and food pattern behavior. Some non-national families may change their feeding pattern when living in countries with high socioeconomic standards, with more consumption of fatty and fast foods.
Table (2). Distribution of the study sample according to overweight and obesity and sociodemographic characteristics.
| Sociodemographic characteristics | Overweight (n= 302) | Obesity (n= 138) | Test of significance & P Value | ||
| No | % | No | % | ||
| Age (years) | |||||
| <16 | 129 | 26.9 | 63 | 13.2 | X32 = 1.17 |
| 16-18 | 173 | 26.5 | 75 | 11.5 | |
| Gender Male | 172 | 30.1 | 88 | 15.4 | X32 = 23.62* <0.05 |
| Female | 130 | 23.1 | 50 | 8.9 | |
| Nationality | |||||
| National | 65 | 20.2 | 34 | 10.6 | X32 = 15.35* <0.05 |
| Non- national | 237 | 29.2 | 104 | 12.8 | |
| Grade | |||||
| 10 | 139 | 30.8 | 69 | 15.3 | X62 = 19.24* <0.05 |
| 11 | 99 | 25.2 | 41 | 10.6 | |
| 12 | 64 | 22.1 | 28 | 9.7 | |
| Mother education | |||||
| Non-educated /low | 40 | 26.1 | 17 | 11.1 | |
| Moderate | 99 | 30.8 | 50 | 15.6 | X62= 12.53 |
| High | 163 | 24.7 | 71 | 10.8 | |
| Family history | |||||
| No | 196 | 25.1 | 88 | 11.3 | X32 = 10.20* ,0.05 |
| Yes | 106 | 30.2 | 50 | 14.2 | |
N.B The cross tabulation involved all categories of BMI percentile but overweight & obesity were only presented.
* P <0.05
Dietary habits are among the factors associated with overweight and obesity among school children. Currently, adolescents have an increasedintake of sweetened beverages, French fries, pizza, and fastfood entrées, including hamburgers, and a consequentlack of recommended fruits, vegetables, dairy foods, whole grains,lean meats, and fish. This change in eating pattern resultsin consumption of excess fat, saturated fat, trans fats, andadded sugars along with insufficient consumption of micronutrients. Peer pressure for conformity, in partdriven by media promotion of fast food directly to teens, makesovereating natural.(36, 37) Students in the present study reported high levels of regular eating of snacks, sweet, fast foods. The present study also demonstrated that eating fast food regularly, was one of the strongest predictors for secondary school students overweight and obesity. This agrees with the results of previous studies. (38, 39) On the other hand, the present study didn’t reveal significant association between regularity of eating breakfast, fruits &vegetables, or sweet and overweight or obesity. Contrary to the present study, the study done at AL- Ain(8), showed that the prevalence of girls who skipped breakfast increased with age, and girls who took breakfast had statistically significant lower prevalence of obesity compared to those who skipped breakfast. Moreover, eating breakfast some days or everyday was protective against obesity only for adolescents with any obese parent.(40)
Table (3). Distribution of the study sample according to dietary habits, life style, and overweight and obesity.
| Item | Overweight (n= 302) | Obesity (n = 138) | Test of significance | ||
| No | % | No | % | ||
| A- Dietary habits | |||||
| Eating breakfast | |||||
| Irregular | 228 | 26.9 | 103 | 12.2 | X32 = 1.72 |
| Regular | 74 | 25.9 | 35 | 12.2 | |
| Eating fruits & vegetables | |||||
| Irregular | 159 | 26.2 | 75 | 12.4 | X32 = 0.20 |
| Regular | 143 | 27.1 | 63 | 12.0 | |
| Eating sweets | |||||
| Irregular | 162 | 25.8 | 81 | 12.9 | X32 = 5.83 |
| Regular | 140 | 27.7 | 57 | 11.3 | |
| Eating snakes & nuts | |||||
| Irregular | 155 | 26.7 | 77 | 13.3 | X32 = 11.79* |
| Regular | 147 | 26.6 | 61 | 11.0 | |
| Soft drink | |||||
| Irregular | 134 | 22.8 | 81 | 13.8 | X32 = 11.44* |
| Regular | 168 | 30.8 | 57 | 10.5 | |
| Eating fast food | |||||
| Irregular | 178 | 24.4 | 82 | 11.2 | X32 = 9.01* |
| Regular | 124 | 30.8 | 56 | 13.9 | |
| B- Life style | |||||
| Physical activity | |||||
| practice >3times/week | X32 = 5.04 | ||||
| No | 147 | 29.7 | 62 | 12.5 | |
| Yes | 155 | 24.3 | 76 | 11.9 | |
| Watching TV/ playing games | |||||
| <2 hours | 78 | 24.0 | 50 | 15.4 | X32 = 6.19 |
| 2 hours or more | 224 | 27.7 | 88 | 10.9 | |
N.B The cross tabulation involved all categories of BMI percentile but overweight & obesity were only presented.
* P <0.05
Several studies (8,20, 30) revealed that low physical activity rates were associated with obesity and television viewing has been shown to be a significant risk factor for pediatric obesity (8,41,42) It was also found that Children who spend more time watching television have a higher BMI and a higher percent of body fat and are less physically active. Watching television can decrease the amount of time spent performing physical activities and has also been associated with increased food consumption either during viewing or as a result of food advertisements. (13) Sedentary behavior (TV viewing) was independently associated with overweight at the age of 8 years in Italy. However, physical activity and energy and nutrient intakes did not significantly affect the change in relative BMI over the four-year period when the parents' obesity was taken into account (43). The present study revealed that near to half of the students were not practicing physical exercise.It also demonstrated that students who were practicing physical activity 3 times/week had a lower but non-significant level of overweight and obesity compared to those who were not practicing. Furthermore, there was no significant association between hours of playing games or watching TV and overweight or obesity. As physical activity in the present study is qualitatively assessed, it may not reflect the exact relation between it and the degree of overweight and obesity.
Table (4). Stepwise logistic regression of the factors affecting the overweight and obesity among secondary school students in Dubai.
| Independent factors | B | SE | OR | 95% Confidence limits LL- UL |
| Eating fast foods | 0.364 | 0.131 | 1.44 | 1.1 – 1.86 |
| Family history of obesity | 0.415 | 0.136 | 1.51 | 1.16 – 1.98 |
| Gender | 0.583 | 0.127 | 1.79 | 1.40 -2.30 |
| Grade of education | ||||
| Grade 11 | 0.096 | 0.170 | 1.10 | 0.78 – 1.54 |
| Grade10 | 0.543 | 0.166 | 1.72 | 1.24 -2.38 |
| Nationality | 0.340 | 0.148 | 1.41 | 1.05 -1.88 |
| Constant | -1.644 | 0.275 | 0.193 |
Reference group: Fast foods :eating fast foods irregularly, family history: no, gender: Female, grade: 12 , nationality: local
LL= lower Limit UL = Upper Limit
Model X62 = 62.68, P<0.05
Literature revealed controversial results concerning the relationship between socioeconomic factors and overweight and obesity. Among the studied factors are socioeconomic level (19, 24, 30,) parental education and occupation (7, 8, 20, 30), and family history of obesity. The present study revealed that mother’s education is not significantly associated with student’s overweight or obesity. Family history of obesity, especially parental obesity, was found to be a strong risk factor for children obesity in most of the studies. (8, 20, 25, 43) Family history of obesity was also found to be a strong predictor for students’ overweight and obesity in the present study.
In conclusion, the present study documented a high prevalence of overweight and obesity among secondary school children in Dubai City. The most important predictors for overweight and obesity among secondary school children are eating fast food regularly, family history of obesity; male gender, being in tenth grade and being non-national students.
6. Conclusion & Recommendation
The high prevalence of obesity among school children in Dubai city and the expected impact on health and health care costs emphasize both the importance of effective strategies to prevent the development of overweight and obesity and the need for community involvement. Health education programs directed to the whole community, especially parents and children, on developing healthy eating patterns should be implemented. Controlling the negative impact of advertising for fast foods in the media over the feeding pattern of the children and adolescents should be emphasized. Implementation of national policies for physical and nutritional education programs in schools is highly recommended. School meal programs should include healthy food choices. Schools should provide training to staff involved in nutrition education with special emphasize on teaching strategies for behavioral change. Schools should involve family and community in supporting and reinforcing nutrition education. Referral of overweight and obese students to diet clinics for proper management should be accomplished to prevent the hazards of obesity on their health status.
References
- Segal DG & Sanchez JC. Childhood obesity in the year 2001. The Endocrinologist 2001; 11 (4): 296-306.
- World Health Organization. Report on Obesity and overweight. Geneva; 2003.
- World Heath Organization MONICA Project, Risk factors. International Journal of Epidemiology 1989; 18 (Suppl 1): S46-S55.
- World Heath Organization. Obesity: preventing and managing the global epidemic. WHO Technical Report Series 894. 2000: Geneva.
- World health organization. Obesity: preventing and managing the global epidemic.
- Report of a WHO consultation on obesity. Geneva, 1998.
- Ruston, D., et al., National Diet and Nutrition Survey: adults aged 19 to 64 years. Nutritional status (anthropometry and blood analyses), blood pressure and physical activity. 2004, Volume 4, 30-32
- Musaiger AO. Overweight and obesity in the Eastern Mediterranean Region: can we control it?. Directorate of Nutritional Studies, Bahrain Centre for Studies and Research, Manama, Bahrain.2004; 10, (6): 789 - 93.
- Kerkadi A, Abo-Elnaga N, Ibrahim W. Prevalence of overweight and associated risk factors among primary female school children in Al-Ain city United Arab Emirates. Emir. J. Agric. Sci. 2005; 17 (1): 43-56
- Caballero B, Himes JH, Lohman TG. Body composition and overweight prevalence in 1,704 schoolchildren from American Indian communities. Am J clin Nutr 2003; Vol. 78, No. 2, 308-312.
- Reilly JJ, Methven E, McDowell ZC, Hacking B, Alexander D & Kelnar CJ. Health consequences of obesity. Archives of Disease in Childhood 2003; 88 (9): 748-52.
- Schwimmer JB, Burwinkle TM & Varni JW. Health related quality of life of severe obese children and adolescents. JAMA 2003; 289 (14): 1813-19.
- Van Horn L, Obarzanek E, Friedman LA, Gernhofer N. Children's adaptations to a fat-reduced diet: the Dietary Intervention Study in Children (DISC). Pediatrics. 2005; 115:1723 –33.
- Giammattei J, Blix G, Marshak HH, Wollitzer AO & Pettitt DJ. Television watching and soft drink consumption: Associations with obesity in 11 to 13 year old schoolchildren. Archives Pediatrics & Adolescent Medicine 2003; 157 (9): 882-86.
- Cornell E .Preventing obesity in youth through school-based efforts, health policy studies division .NGA centre for best practices, 2003.
- CDC (2000) growth charts for the United States methods and development series report 11, No. 246: 201.
- Feinstein AR. Principles of medical statistics. 1st edition. Boca Raton, London, New York: Chapman & Hall / CRC. A CRC press company. 2002.
- Jekel JF, Katz DL, Elmore JG. Epidemiology, biostatistics and preventive medicine. 2ed editions. Philadelphia, London. New York: WB Saunders Company.2001.
- World Health Organization (WHO). Obesity, Preventing and Managing the Global Epidemic. Report of a WHO Consultation on Obesity, Geneva, 1997.
- Vieweg VR, Johnston CH, Lanier JO, Fernandez A, Pandurangi AK.Correlation between high risk obesity groups and low socioeconomic status in school children. South Med J. 2007; 100(1):8-13.
- De Vito E, La Torre G, Langiano E, Berardi D, Ricciardi G. Overweight and obesity among secondary school children in Central Italy.European Journal of Epidemiology 1999; 15(7): 649-54
- Al Isa AN. Dietary and socioeconomic factors associated with obesity among Kuwaiti college men. Br. J. Nutr. 1999; 82:369-74.
- Kim, S., S. Moon and B. M. Popkin. The nutrition transition in South Korea. Amer. J. Clin. Nutr. 2000; 71:44-53.
- El- Hazmi, M. A. F. and A. S. Warsy. A comparative study of prevalence of overweight and obesity in children in different provinces of Saudi Arabia. J. Trop. Pediatrics 2002; 48:172-77.
- Al-Saeed WY, Al-Dawood KM, Bukhari IA, Bahnassy A. Prevalence and socioeconomic risk factors of obesity among urban female students in Al-Khobar city, Eastern Saudi Arabia, 2003. Obes Rev. 2007 ; 8(2):93-9.
- Musaiger AO, Matter AM, Alekri SA, Mahdi AR. Obesity among secondary school students in Bahrain. Ministry of Health, Bahrain ,Nutrition Unit, Public Health Directorat. 1993
- Malik M., Bakir A. Prevalence of overweight and obesity among children in the United Arab Emirates. Obesity Reviews 2007 ;8 (1), 15–20.
- Al Haddad FY, Al-Nuaimi BB, Thabit M. Prevalence of obesity among school children in The United Arab Emirates. Amer. J. Human. Biol. 2000; 12:498-502.
- Badrinath P, Al-Shboul QA, Zoubeidi T, Gargoun AS, Gubash R, El-Rufaie OE. Measuring the Health of the nation. United Arab Emirates Health and Life style Survey;2000.
- Humeníkova L, Gates GE. Dietary intakes, physical activity, and predictors of child obesity among 4-6th graders in the Czech Republic. Cent Eur J Public Health. 2007; 15(1):23-8.
- Mozaffari H, Nabaei B. Obesity and related risk factors. Indian J Pediatr. 2007 ;74(3):265-7.
- Kasmini K, Idris MN, Fatimah A, Hanafiah S, Iran H & Asmah Bee MN. Prevalence of overweight and obese school children aged between 7 to 16 years amongst the major 3 ethnic groups in Kuala Lumpur, Malaysia. Asia Pacific Journal of Clinical Nutrition 1997; 6(3): 172-174.
- Chhatwal J, Verma M, Riar SK. Obesity among pre-adolescent and adolescents of a developing country (India). Asia Pac J Clin Nutr. 2004; 13(3):231-5
- The National Eating Disorder Information Centre, Discover Healthy Eating! A Teacher’s Resource for Grades 1-8, 2000 .Cited at May 2007. Available from http://www.toronto.ca/health/he_bg_all.pdf.
- Mohammadpour-Ahranjani B, Rashidi A, Karandish M, Eshraghianand MR, Kalantari N.Prevalence of overweight and obesity in adolescent Tehrani students, 2000–2001: an epidemic health problem. Public Health Nutr. 2004; 7(5):645-8
- Ismail MN, Tan CL. Prevalence of obesity in Malaysia. Country Report at the Regional Advisory Meeting on Obesity. August 1998. Manila, Philippines.
- Bowman SA, Gortmaker SL, Ebbeling CB, Pereira MA, Ludwig DS. Effects of fast-food consumption on energy intake and diet quality among children in a national household survey. Pediatrics. 2004;113 :112 –18
- Putnam J, Allshouse J, Kantor L. U.S. Per Capita Food Supply Trends: More Calories, Refined Carbohydrates and Fats. Washington, DC: Economic Research Service, US Department of Agriculture;2002.
- Muller, M. J., I. Koertringer, M. Mast, K. Languix and A. Frunch. Physical activity and diet in 5 to 7 year old children. Public. Health. Nutr. 1999; 2:443- 44.
- Robinson, TN. Reducing children's television viewing to prevent obesity: randomized controlled trial. JAMERA. 1999; 282:1561-67.
- Fiore H, Travis S, Whalen A, Auinger P, Ryan S. Potentially protective factors associated with healthful body mass index in adolescents with obese and nonobese parents: a secondary data analysis of the third national health and nutrition examination survey, 1988-1994. J Am Diet Assoc. 2006; 106(1):55-64
- Hanley AJ, Harris GSB, Gittelsohn J, Wolever TM, Saksvig B, Zinman B.. Overweight among children and adolescents in Native Canadian community: prevalence and associated factors. Amer. J. Clin. Nutr. 2000; 71:693-700.
- Coon KA, Goldberg J, Rogers BL, Tucker KL. Relationships between use of television during meals and children’s food consumption patterns. Pediatric2001; 107:167-76.
- Maffeis C, Talamini G, Tatò L. Influence of diet, physical activity and parents' obesity on children's adiposity: a four-year longitudinal study. Int J Obes Relat Metab Disord. 1998; 22(8):758-64.



