
International Journal of Preventive Medicine Research, Vol. 1, No. 4, October 2015 Publish Date: Jul. 16, 2015 Pages: 186-192
Effect of Health Education Interventions on Women Knowledge, Attitude, and Practice of Malaria and on Malaria Morbidity and Mortality Rate: An Experimental Study
Maha Hamad Mohamed Ali1, Hatim Rahamtalla Mohamed Ahmed2, Fatima Fadul Ali Osman1, Osman Babiker Osman1, *
1Health Education Department, Public Health Faculty, Alzaiem Al-Azhari University, Khartoum, Sudan
2Health Education Department, Public Health Faculty, Bahari University, Khartoum, Sudan
Abstract
Background/objective: Malaria is a leading cause of morbidity and mortality in the developing countries. In endemic areas, malaria infection during pregnancy accounts for up to a quarter of all cases of severe maternal anaemia, and for 10-20 percent of low birth weight babies. This study aimed to assess the effect of health education interventions (Information, Education and Communication (IEC), and Behavior Change Communication (BCC)) on pregnant women knowledge, attitude and practice for malaria and the malaria morbidity and mortality rate among both pregnant women and women with under-five children. Methods: This is a quazi-experimental study. It was conducted among 400 participants selected randomly from eight villages from East Gezira Locality. Training sessions in health education strategies were held targeting community health workers from the target area. Those trainees conducted the interventions that based on different health education strategies continued for one year. The data were collected before and after intervention, compared and analyzed, using SPSS and chi square test. Results: The result revealed that, there is a significant increase in knowledge, since where there are significant increases in knowledge concerning mosquito types from 46.7% to 92.2%, malaria mode of transmission from 35.4% to 81.5% and concerning consequences of malaria from 43.2% to 83.8%.The attitude of mothers towards the daily usage of insecticide treated nets has improved significantly after the intervention from 6.2% to 99.5%. There was also a significant promotion of practices concerning the use of integrated treated nets from 26.8% to 81.5%.Malaria morbidity rate significantly decreased after the intervention from 24.3%to19.10% and the mortality rate significantly decreased after the intervention. Conclusion: It could be concluded that the health education interventions yield good result in increasing knowledge, improving attitudes and practices which in turn reduce morbidity and mortality rate of malaria among the pregnant women.
Keywords
Health Education, Women, Knowledge, Attitude, Practice, Morbidity, Mortality, Malaria
Received:April 26, 2015
Accepted: May 13, 2015
Published online: July 15, 2015
@ 2015 The Authors. Published by American Institute of Science. This Open Access article is under the CC BY-NC license. http://creativecommons.org/licenses/by-nc/4.0/
1. Introduction
Malaria is the leading cause of morbidity and mortality in developing countries. Nearly half a billion people contract malaria each year, more than a million people dieannually (1). Children under five and pregnant women represent a large portion of the population at risk. In endemic areas, malaria during pregnancy accounts for up to a quarter of all cases of severe maternal anemia, and for 10-20 percent of low birth weight babies, it is the most malaria-related deaths occur in Africa, (2).
Each year, approximately 25 million African women become pregnant in the malaria-endemic areas and are at risk of plasmodium falciparum malaria during pregnancy, most women in the regionreside in areas of relatively stable malaria transmission where the principal effects of malaria infection during pregnancy are associated with malaria-related anemia in mothers and with the presence of parasites in the placenta, (3).
Malaria is more dangerous to pregnant women because the parasites cause pregnant women to become weak and anemic that can lead to death during delivery if the mother suffers from complications that cause a lot of bleeding. Severe malaria in pregnancy is a medical emergency requiring referral to hospital where intensive care can be offered. Malaria in pregnancy can easily be diagnosed, treated and prevented (4).
Malaria is a public health problem in Sudan, presenting a heavy burden to the national economy and health services, as 22% of labor time is lost due to malaria. About 98% of the population at risk formalaria, 40% of the outpatients’ attendance is due to malaria. In Sudan malaria causes one death every 50 minutes (1). Around 4 million of malaria cases occurred among children less than 5 years old admitted to hospital for treatment (2).
Information, Education and Communication (IEC) is defined as an approach which attempts to change or reinforce a set of behaviors in a target audience regarding a specific problem in a predefined period of time,(5).Itis the best way to change individual and community attitudes and practices that act as barriers to effective malaria control, through multi-channel communication, including interpersonal, community, electronic and print media (6). IEC is a process of working with individuals, communities and societies to develop communication strategies to promote positive behaviors which are appropriate to their settings, (7). IEC is important in delivering messages to control and prevent malaria among pregnant mothers through proper malaria preventive massages, (8).Behavior Change Communication (BCC)is a multi-level tool for promoting and sustaining risk reducingbehavior change in individuals and communities by disseminating research based and targeted messages, using a variety of channels. The Purpose of Behavior Change Communication is to transfer messages using an appropriate channel in order to influence the audience behaviours. Communication is essential to communicating policy changes, home based management, improving the quality of health care, creating demand for malaria services and products, changing household practices, and mobilizing communities for malaria control (6).
Gezira State is one of the most hyper endemic malaria areas in Sudan, due to the presences of wide irrigation schemes (10,000Km2). The selected 8 villages in the East Gezira locality lie along large rice scheme that sustain a lot amount of water throughout the area, hence favoring sustainable mosquito vector breeding sites.In endemic areas, malaria infection during pregnancy accounts for up to a quarter of all cases of severe maternal anemia, and for 10-20 percent of low birth weight babies.There were no traced malaria interventions in Sudan using the approach of changing behavior through IEC and BCC strategy. Malaria can easily be prevented by changing behavior through IEC and BCC strategy intervention.Therefore, this study aimed to assess the effect of health education interventions (Information, Education and Communication (IEC), and Behavior Change Communication (BCC)) on pregnant women knowledge, behavior and practice formalaria and the malariamorbidity and mortality rate among the pregnant women and under five children.
2. Materials and Methods
A quasi-experimental study designed was conducted during the 2011-2013, targeted pregnant women and under five children in the Eastern Gezira Locality with the aim to find out the best intervention to decrease malaria morbidity and mortality rate and improving the pregnant women knowledge, behavior, and practice for malaria.
This study conducted inEastern Gezira locality is the biggest locality in Gezira State, is bordered by Khartoum state from the north, Blue Nile at west and Gaderif state at east.The locality occupied 1800 km2, hosted about 78 thousand population, the locality has 72 villages, eight of themwere the study area, and these villages were reported as a high malaria endemic area in the locality. The Eastern Gezira locality has a population about 78 thousand. The total pregnant women in the locality were about (674) and children under five years were (1692). Pregnant women and mothers with at least one child under five years of age were the study population.
The study population was the pregnant woman and women with under-five children, hence the total households were found to be 13945.Therefore the sample size was calculated to be 400 pregnant women andwomen with under-five children.The following formula was used to calculate sample size n=4pq/l2. The State was chosen purposefully as it is a malaria endemic State in Sudan. The Eastern Gezira locality was chosen randomly. It has 72 villages, eight of which was chosen for study randomly. The sample was selected from each village proportionally, using systematic random sampling techniques.
The ethical approval was obtained from the ethical committee of AlziemAlazhari University, Sudan. Different methods were used to collect data, including questionnaires, focus group discussion, and observational checklist.
The intervention consists of three phases; pre-intervention phase, introductory phase: included: Many meetings were held with the concerned community leaders, authorities gain ethical clearance, political and technical support. Training sessions were conducted, intervention materials were prepared, and a pre-test was carried out using questionnaire, observation checklists and focusing group discussions, the Intervention phase, after a two day training session (8 hrs.), targeting community health workers. The trainees have conducted the intervention which includes; intra and interpersonal communication, messages concerning malaria, encouraging using insecticide treated nets (ITNs), changing behaviours. The intervention has continued forone year, and post-intervention phase, a post- test was carried out, after two months of the end of the intervention, by using the same pre-test questionnaire, observation checklists and focusing group discussions to collect data after the intervention. The indicators were; Changes in knowledge, attitudes and practices, malaria morbidity, mortality rate among pregnant women and mothers with children under 5 years old.
The data that collected before and after the intervention was compared by using chi-square test and analyzed by computer using the SPSS software program, version 20.
3. Results
The results revealed that the average age of respondents is 27.5 years, almost all the participants are literacy (97.25%), and the range of family size of households is about 5-6 individuals and the majority of respondents (94.2%) were housewives who were not engaged in any work.
Knowledge: The result revealed that there were slight increases in knowledge concerning malaria vector from 98.5% to 100%, types of insect transmitting malaria from 97.3% to 100%, where there are significant increases in knowledge concerning mosquito types from 46.7% to 92.2%, malaria mode of transmission from 35.4% to 81.5%, (Figure 1). Knowledge concerning the consequences of malaria infection during pregnancy increased significantly after the intervention from 43.2% to 83.8%, (Figure 2).
Attitudes: The result revealed that there was insignificant improved of attitudes towards the consequence of malaria during pregnancy after the intervention from 99% to 99.80, (Figure 3), Where the attitude of mothers towards the daily usage of ITNs have improved significantly after the intervention from 6.2% to 99.5%. Feeling of protection with ITNs possession has also improved significantly from 86.5% to 99.8%, (Figure 4).
Practice: The results revealed that there was a significant promotion of practices concerning the use of ITNs on sustainable or continuous order increased significantly after the intervention from 26.8% to 81.5%, the daily practice to ensure that their children sleep under the net from 53.5% to 98.5%, (Figure 5).
Morbidity and mortality rate: Malaria morbidity rate decreased significantly after the intervention from 24.3% to 19.10%, (Figure 6) and the mortality rate decreased in significantly after the intervention from 3.1% to 1.40%, (Figure 7).
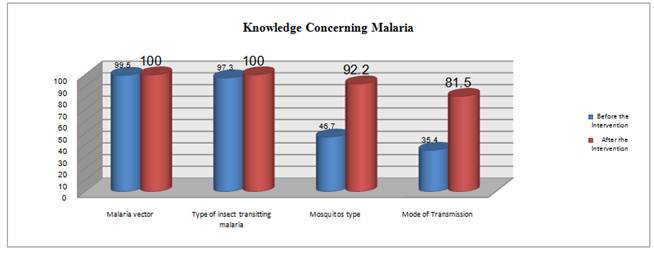
Figure (1). The effect of health education interventions on knowledge levels of the participants concerning malaria in East Gezira Locality, Sudan, 2013: n=400.
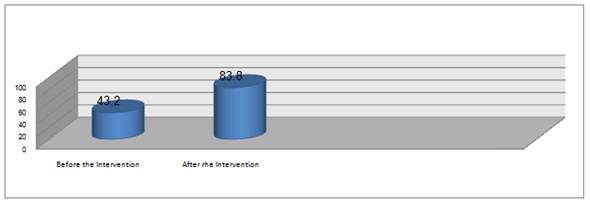
Figure (2). The effect of health education interventions on knowledge of consequences of malaria infection during pregnancy in East Gezira Locality, Sudan, 2013: n=400.
Knowledge about malaria vector increased significantly after the intervention from 98.5% to 100%. λ2 = 0.019 df=1 P value (0.038). Knowledge about insect transmitting malaria increased insignificantly after the intervention from 93.7% to 100%. λ2 = 0.0353 df =1 P value (0.0405). Knowledge about mosquito types increased significantly after the intervention from 46.7% to 92.2% λ2 = 176.91df =3 (P value =0.000).
Knowledge about the malaria mode of transmission increased significantly after the intervention from 35.4% and 81.5%. λ2 = 176.91df =3 (P value =0.000).
Knowledge about the consequence of malaria during pregnancy increased significantly after the intervention from 43.2% to 83.8%. λ2 = 145.51df =4 (P value =0.000)
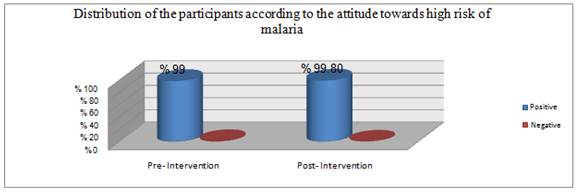
Figure (3). The effect of health education interventions on participants’ attitude towards high risk of malaria in East Gezira Locality, Sudan, 2013: n=400.
Attitudes about the consequence of malaria during pregnancy improved insignificantly after the intervention from 99% to 99.80%. λ2= 0.3050 df =1 (P value = 0.37)
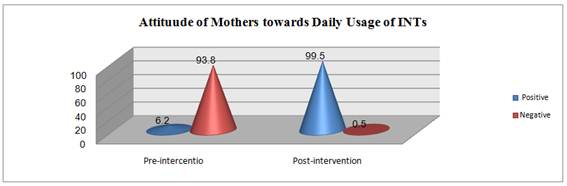
Figure (4).The effect of health education interventions on participants attitude towards the daily usage of ITNs in East Gezira Locality, Sudan, 2013: n=400.
Attitude of Mothers towards the daily usage of ITNsimproved significantly after the intervention from 6.2% to 99.5%. λ2= 894.21, degree of freedom = 1, P value = 0.000
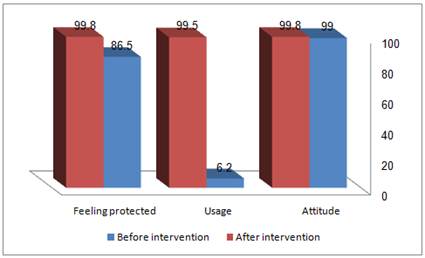
Figure (5). The effect of health education interventions on participants’ attitude, usage and feeling protected of using ITNs on sustained or continuous order in East Gezira Locality, Sudan, 2013: n=400.
Practice concerning using ITNs on sustained or continuous order increased significantly after the intervention from 26.8% to 81.5%. λ2 = 239.25df =1 P value (0.000)
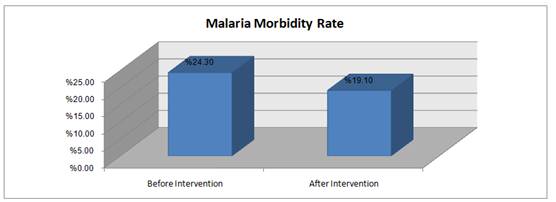
Figure (6). The effect of health education interventions on malaria morbidity rate in East Gezira Locality, Sudan, 2013: n=400.
The malaria morbidity rate decreased significantly after the intervention from 24.3%to19.10%.λ2= .023, degree of freedom = 1, P value = 0.013
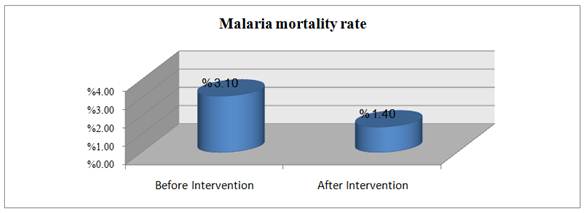
Figure (7). The effect of health education interventions on the malaria mortality rate in East Gezira Locality, Sudan, 2013: n=400.
The malaria mortality rate decreased significantly after the intervention from 3.1%to1.40%. λ2= .003, degree of freedom = 1, P value = 0.013
4. Discussion
This study found that literacy is a predominant feature of the participants as 97.7% were engaged in formal education. The average age was 27.5% years, these demographic variables were confirmed to influence the utilization of ITN in a study conducted by SaadEldeenHussien et al, 2008 in Eastern Sudan, where it was observed that educated individuals sleep more under the net, and letting more under-fives and pregnant women sleep under the net. Also, Julie, 2010, in his study conducted in Kinshasa, Congo, found that education level of family head of household is a major factor affecting the use of ITNs (9).
Knowledge; after the health education interventions, IEC and BCC strategies, have been held in the area, the level of malaria related knowledge was found to increase, where knowledge concerning mosquito types increased significantly from 46.7% to 92.2%, malaria mode of transmission from 35.4% to 81.5%. Knowledge concerning the consequences of malaria infection during pregnancy increased significantly after the intervention from 43.2% to 83.8%. This increased ITNs utilization and lead to the reduction in mortality and morbidity rate among the participants. This finding agrees with the study that conducted by Amina in 2008, in El Hosh, South Gezira State, She concluded that improved knowledge, attitude and practices (KAP) lead to increase the utilization of ITNs as a result of Health Education interventions (10).
Another study conducted by Ssenganzi and Makumbi, in Uganda among 202 households having children under five from July 2006 to January 2007. The study aimed at examining the role of malaria health education provided by trained community health workers (CHWs) in increasing the rate of ITNs utilization and reduction of malaria burden among children under five. The study concluded that a significant drop in the incidence of malaria in children under five was reported in the area having a malaria education comparable to that received ITNs without health education (11).
The severity of malaria during pregnancy was identified by only 43.2%, similar finding was explored by malaria division in Kenya in their KAP survey conducted in 2004. After the intervention this become83.8% study showed that only one quarter of mothers perceived malaria during pregnancy as serious. ITNs use is mentioned by 26.8% before intervention and increased to 81.5% after, the difference is statistically significant (P. value = 0.001), this means the intervention led to a significant increase in ITNs use (12).
Perceived advantages and disadvantages play a role in ITNs utilization, the study described benefits mentioned by the participants as 23.9% prevent mosquito contact, 41% kill mosquito, the disadvantages were almost negligible, (29.4%) perceived allergy, (25.6%) curb and lack of customization (29%), these reasons had been modified significantly after the intervention. Similar studies cited the same advantage and negative attitude, net mark in Ethiopia, 2004 reported that the vast majority (90%) stated that ITNs kills mosquito and 40% repel (13).
The study concluded that health education strategies IEC and BCC found to be effective in increasing knowledge, improving attitudes and promoting practices concerning malaria. These changes in knowledge, attitudes and practices tend to reduce malaria morbidity and mortality rate among the participants. The malaria control administration has to use communication strategies as integral with other strategies as vector control and malaria management protocol.
Acknowledgement
We are grateful to allparticipants in this study.
References
- Republic of Sudan FMOH, National Strategic Plan for Roll Back Malaria 2001-2010. 2011.
- Republic of Sudan FMOH, National Malaria Control Program Sudan, National Malaria Indicator Survey 2009.
- Root, G., Collins, A., Munguti, K., Sargent, K. Roll Back Malaria Scoping Study, Malaria Consortium, Kampala, Uganda, 25 April 2003.
- WHO. The Global Malaria Action Plan, WHO, Roll Back Malaria, WHO, Geneva, 2008.
- Simon J, Larson B, Zusman A, Rosen S. How will reduction of tariff and taxes on insecticide treated mosquito nets affect household purchases. Bulletin of the World Health Organization.2008; 80(11): 892-899.
- Chard E. Gbulskis, John Miker, Monitoring Mosquito Net Coverage for Malaria Control in Africa Tropical and International Health, Vol. 8, pp 693-703, August 2003.
- laii JA, Hawley WA, Kolczak MS, Terkuile FO, Gimnig JE, Vulule JM, et al. Factors affecting use of permethrin-treated bed nets during a randomized control trial in western Kenya. Am J Trop Med Hyg. 2003;68(4):137-141
- Deressa W, Chibsa S, Olana D. The Distribution and Magnitude of Malaria in Oromi, Ethiopia. Ethiopian Journal of Health Development.2004;18(3):164-70.
- SaadEldienHussien,Elfatih Malik, Soumiaokoued and Elsadig M Eltayeb, Retention and Efficacy of ITNs Distributed in EASTERN Sudan: a two –step community-based study, Malaria Journal 2008.
- Amina,A. The role of health education in promoting the utilization of ITNs among pregnant mothers in Elhosh –South Zegira- Sudan, 2008.
- RBM, Insecticide-Treated Mosquito Net Interventions, A manual for national control programme managers, Geneva, 2003.
- Sengonzi R. and Makumbi,F., Assessing the Effect of Combined Malaria Prevention and Education and Free ITNs on self-reported malaria among children in Northern Uganda -RTI Press, Uganda 2010.
- Deressa W, Chibsa S, Olana D, Magnitude of Malaria Admissions and Deaths at Hospitals and Health Centers in Oromia, Ethiopia. Ethiopian Medical Journal.2004; 42 :237-46.



