
Clinical Medicine Journal, Vol. 1, No. 2, June 2015 Publish Date: Apr. 22, 2015 Pages: 38-42
Nutritional Anemia Among Patients Referred to Hematology Laboratories in Port Sudan City
Munsoor Mohammed Munsoor1, *, Mohammed Omer Gibreel2, Mubarak El Saeed El Karsani3
1College of Medical Laboratories, Sudan University of Sciences and Technology, Khartoum, Sudan
2Department of Hematology, Port Sudan Ahlia College, Port Sudan, Red Sea State, Sudan
3College of Medical Laboratories, Kararry University, Omdurman, Sudan
Abstract
This is a descriptive study conducted in Port Sudan city (2012-2014) to evaluate the prevalence of nutritional anaemia among 600 patients referred to hematology laboratories in three major hospitals. The patients composed of 382 (63.7%) females and 218 (36.3%) males with a mean age of 31 years. The results showed that, the mean values of hemoglobin and serum iron in study population were 10.6 g/dl and 55.6 mg/dl respectively.The serum iron concentration was normal in 406 (67.9%), low in 92 (15.3%) (iron deficiency anaemic patients) and within lower limits of normal in 102 (16.8%) of the patients. Among the 92IDA patients, 74 (80.4%) were in the adult group (19-85 years) and 3.1% of the population showed iron deficiency without anaemia. The results of the peripheral blood films revealed that, 338 (56.3%) of the smears were normocytic normochromic, 230 (38.3%) showed microcytic hypochromic cells, 19 (3.3%) showed marked anisopoikilocytosis and 13 (2.2%) showed microcytosis with pencil cells. Normal morphology of white blood cells was seen in 81.7% of smears, leukocytosis in 15.7% and leucopenia in 2.7% while adequate platelets were seen in 82.2%, thrombocytosis in 13.7% and thrombocytopenia in 4.2%. This study concluded that, IDA was prevalent among the study subjects and children althoughthe elder patients were the most affected group.The study strongly recommended the conduction of a national nutritional survey including collection of data on iron status and prevalence of anaemia in all groups of the population in the area of study.
Keywords
IDA in Sudan, Anaemic Patients, Serum Iron, Port Sudan
Received: March 24, 2015
Accepted: April 6, 2015
Published online: April 20, 2015
@ 2015 The Authors. Published by American Institute of Science. This Open Access article is under the CC BY-NC license. http://creativecommons.org/licenses/by-nc/4.0/
1. Introduction
Anemia is a global health issue that has significant consequences for individual health and socioeconomic development. It is defined by haemoglobin (Hb) concentration below 11g/dl. This results in insufficient oxygen delivery to tissues and organs(1). It is a widespread public health problem associated with an increased risk of morbidity and mortality; especially in pregnant women and young children(2). Nutritional anaemia is a recognized public health problem throughout the world. An estimated 30 percent of the world’s population is anaemic, with the global prevalence of anaemia among 6-12 years old children to be 36 percent and 77 percent in developing regions respectively(3). Nutritional anaemia is worldwide distributed; approximately 20 percent of women, 50 percent of pregnant women, and 30 percent of men are iron deficient. Iron is an essential component of haemoglobin, the oxygen carrying pigment in the blood and is normally obtained through the food in the diet and by the recycling of iron from old red blood cells(4). Iron deficiency anaemia occurs in 2 percent to 5 percent of adult males and postmenopausal women in the developed world. Iron deficiency with or without anaemia, is even more frequent(2,5).Possible causes of anemia include haemolysis occurring with malaria, glucose-6-phosphate dehydrogenase deficiency, congenital hereditary defects in haemoglobin synthesis, and deficits in other nutrients, e. g. vitamins A, B12, and C, and folic acid(6).Nutritional anemia, including iron deficiency anemia (IDA), is one type of anemia that prevalent in Sudan and caused by limited consumption of meat(7). In 1995, nutritional anemia was among the ten major causes for hospital admission in Sudan. However, nationally representative data on iron deficiency were limited in the country. In 1997 WHO reported that, the prevalence of anemia in Sudanese children under five years was high and more than 80% of children were anemic. In Khartoum the prevalence was the lowest but affected almost one third of children(7). In 2003, in the crisis-affected population of Darfur, the prevalence of anemia was 55%(4). But reports concerning IDA in Sudan were rare. In 2012, in a study in Khartoum hospital, the prevalence of IDA among Helicobacter pylori infected and uninfected Sudanese pregnant women were reported to be 11%(8) and 74%(9) respectively. Because there was no report for the status of IDA in Eastern Sudan, this study was undertaken to determine the prevalence of nutritional anemia among patients referred to major three hospitals in Port Sudan city, Red sea State.
2. Material and Methods
2.1. Study Design and Objective
This is a noninterventional, descriptive cross sectional study conducted to determine the prevalence of iron deficiency anemia among patients referred to hematology laboratories in Port Sudan city. The study was conducted in Police Hospital, Sea Ports Corporation Hospital and Hematology department in the central laboratory.
2.2. Study Population and Sampling
The subjects enrolled for this study were 600 of both sex and suspected to have anemia, their ages ranged between 1year and 85 years. A stratified multi-stage probability sampling methodology was used in selecting the study population. Five ml of venous blood was withdrawn from each of the 600 randomly selected participants under anti septic condition. Then 2.5 ml was kept in lithium heparin anticoagulant container to obtain plasma for iron testing and other 2.5 ml was collected in EDTA for complete blood count.
2.3. Laboratory Analysis
The complete blood count was performed by the XE 2100 hematologyanalyzer according to the RF/DC detection method, hydrodynamic focusing (DC detection), flow cytometry and SLS-haemoglobin method following the instructions supplied by the manufacturer.Plasma iron wasanalyzed based on the principle that transferrin-bound ferric irons in the sample are released by guanidinium and reduced to ferrous by means of hydroxylamine. Ferrous iron reacts with ferrozine forming a color complex that can be measured spectrophotometrically. The reference values considered for plasma iron were 65-175 µg/dl = 11.6-31.3 µmol/l for male and 50-170 µg/dl= 9.0-30.4 µmol/l for female.
2.4. Ethical Consideration
The information obtained from participants was coded and stored in computers accessible only to the investigators and doctors supervising the treatment of the patients. All participants were interviewed, personal details were recorded into questionnaires and verbal consent was obtained at the enrolment of each participant.
2.5. Statistical Analysis
Data entry and statistical analysis was performed using the SPSS version 11.5 program. Descriptive data are presented as percentages or as means± SD. Chi-square test was performed to detect any association between anemia prevalence and independent variables. Mann-Whitney U and Kruskall Wallis tests were used in making comparisons between the red blood cell indices. A p value of < 0.05 was considered statistically significant. Backward logistic regression analysis was performed to evaluate the independent association existing between the potential risk factors and anemia. Independent variables that were significant at the p = 0.05 level in univariate analysis were included in multivariate analysis to control for confounding factors in regression models. The results were presented in odds ratios (OR) and 95% confidence intervals. Hb < 11.0 g/dl was considered anemia for general sample while doing the statistical analysis.
3. Results
This descriptive study was conducted in Port Sudan city and aimed at the determination of serum iron concentration in anaemic patients in Port Sudan. The study included 218 (36.3%) male and 382 (63.7%) female patients aged between 1 year and 85 years with the mean age being 31 years. The result of this study revealed that, the mean hemoglobin concentration in the study group was 10.6 g/dl andthe mean serum iron concentration was 55.6 mg/dl (table1). The serum iron concentration was normal in 406(67.7%), low in 92 (15.3%) and within lower limits of normal in 102 (16.8%) of the patients (table 1).Among the study population, 92 (15.3%) individuals showed iron deficiency anaemia and 18 (3%) showed low serum iron without anaemia. Out of the 92 patients with iron deficiency anaemia, 12 (13%) were children (aged between 1-12 years), 6 (6.6%) were adolescents (13-18 years old), and 74 (80.4%) were adults (More than 18 years old). No significant difference was seen between males and females in the Hb concentration (p. value = 0.207) but the difference was significant between the two groups in the serum iron concentration (p. value = 0.033) (table 2). The Hb concentration in the study group was neither affected by age nor by sex. Serum iron concentration was significantly associatedwithage and sex (p. value= 0.033). Blood films revealed that, 338 (56.3%) of the peripheral blood smears were normocytic normochromic, 230 (38.3%) of blood smears showed microcytic hypochromic cells, 19 (3.3%) showed marked anisopoikilocytosis and 13 (2.2%) smears showed microcytosis with a relative numbers of pencil cells. Normal morphology of white blood cells was seen in 81.7% of cases, leukocytosis in 15.7% and leucopenia in 2.7% while adequate platelets were seen in 82.2% of cases, thrombocytosis in 13.7% and thrombocytopenia in 4.2% (table 3).
Table 1. Serum iron level among study subjects.
| Level of serum iron | No. of females | No. of males | Total | Mean of iron (all patients) |
| Low | 053 | 039 | 092 | 55.6 mg/dl |
| Within lower limit | 061 | 041 | 102 | |
| Normal | 268 | 138 | 406 | |
| Total | 382 | 218 | 600 |
Table 2. Mean values for the CBC and serum iron in the study group as assessed by Chi square.
| NO | Items | Males | Female | P. value |
| 1 | Hb g/dl | 11 | 10.4 | 0.207 |
| 2 | RBCs count mg/dl | 4.41×106 | 4.2×106 | 0.000 |
| 3 | Serum Iron mg/dl | 51 | 58.2 | 0.032 |
| 4 | Hct L/L | 35 | 33.5 | 0.017 |
| 5 | MCV Fl | 77.6 | 79.2 | 0.117 |
| 6 | MCH Pg | 25.7 | 26.4 | 0.677 |
| 7 | MCHC/µl | 31.4 | 31.2 | 0.211 |
| 8 | WBCs/µl | 8.3×103 | 9.2×103 | 0.649 |
| 9 | Plt count/µl | 322×103 | 295×103 | 0.022 |
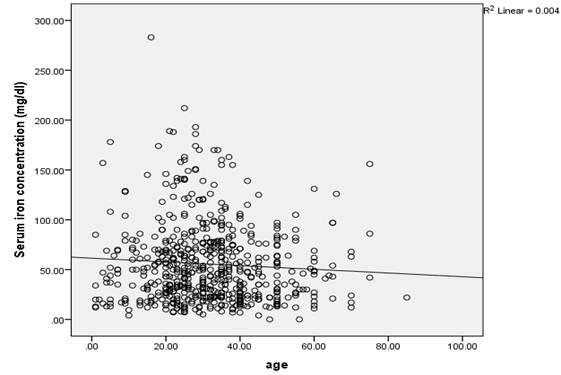
Figure 1. Scatter diagram showing the negative correlation between serum iron concentration and age. Most of the study population clustered between 16 and 45 years of age.
Table 3. Morphology of RBC, WBC and platelets status as observed for each type of cell into the 600 blood smears of study subjects.
| Type of blood cells | Morphology | Percentage of smears |
| RBC | Normocytic normochromic | 56.2% |
| RBC | Microcytic hypochromic | 38.3% |
| RBC | Anisopoikilocytosis | 03.3% |
| RBC | Microcytosis with pencil cells | 02.2% |
| WBC | Normal morphology | 81.6% |
| WBC | Leukocytosis | 15.7% |
| WBC | Leucopenia | 02.7% |
| Platelets | Adequate | 82.2% |
| Platelets | Thrombocytosis | 13.6% |
| Platelets | Thrombocytopenia | 04.2% |
4. Discussion
The present study was conducted in port Sudan city Red Sea State in Sudan to assess the status of nutritional anemia among the individuals of that State. The prevalence of IDA (defined as serum ferritin level <15µg/l(6)) was found to be 15.4%. The majority of affected individuals were among the adults (above 18 years) age group which constitutes 80.4% of the study population, followed by children (1-12 years) (13%) and adolescent (13-18 years) (6.6%). Anemia (defined as hemoglobin<11.0 g/dL) is still a worldwide problem especially among children and women in the child bearing age. Anemia may be predisposed due to several factors that deplete iron level in the blood stream. Such factors include define risk factors (age, gender, pregnancy, physiological state, socioeconomic and nutritional status) and diseases. However, no report of IDA status among the whole Sudanese population during the last 9 years was issued. The result of the current study reflected the IDA prevalence in Red Sea State and not be representative for the Sudan as a whole. This because that state is a marginal region with modernized life style and the health awareness is highly adopted in that region compared with other parts of the country. On the light of the present result, the IDA prevalence in the study region was lower than that reported in Iran (43.4%), Philippines (28%), Mexico (24.17%) but higher than that reported in South Korea (0.7%)(10-13). In the studying of the relation between the serum iron and age, the result shows that most of the study populations were in adult group and the serum iron on this group has the most lower level compared with children and elders. This conclusion is in contradiction with former report that the most IDA-affected age groups were children and elder people(14). The disagreement may be due to low intake of iron enrich food by the adult people. Because Sudanese people at this age preferred to feed their children and elder relatives on expenditure of their own requirements when the resources became scares in the country. Also because people at this productive age were much more susceptible to parasitic infection that cause blood lost and GI bleeding of unknown etiology. This is supported the reports that low income, iron- or vitamin C-poor diets were also associated with IDA(15).The peripheral blood morphologic findings in our work provided a quantitative support topoikilocytes (known as prekeratocytes) and pencil cells as morphologic features of IDAand provide evidences for use of peripheral cell morphology as a means of differential diagnosis for various types of anemias(15,16).Our results of peripheral blood demonstrate hypochromic, microcytic red blood cells and also indicated association of IDA with anisopoikilocytosis a feature which has been reported earlier(16). Furthermore, the blood film in the present study observed normal morphology of white blood cells, leukocytosis, leucopenia, adequate platelets, thrombocytosis and thrombocytopenia in association of IDA. These results may be of value in further diagnosis of microcytic anemias.This study recommended that, for populations with defined risk factors in terms of age, gender, physiological state and socioeconomic and nutritional status, national health policy to reduce IDA is needed. This study concluded that nutritional anemia is still a major problem in Red Sea State in Sudan.
References
- El-zammar D, Yan M, Huang G, Fang D, Petigura F, Bornn L, Ngai T, Brkanovic S, Khangura J, Alexander N, Hendry S, Lubin J, Wallis C, Ford J, Kapoor V. Assessment and management of anemia in a population of children living in the Indian Himalayas: A student-led initiative. Global Health Initiative. 2011; 2: PP. 12, 13.
- Mc Lean E. Cogswell M, Egli I, Wojdyla D, deBenoist B.Worldwide prevalence of anemia in preschool aged children, pregnant women and non-pregnant women of reproductive age. In: Kraemer K. and Zimmermann M. B. Nutritional anemia. Switzerland: Sight and Life, 2007: P 2.
- Gomber S.Madan N, Lal A, Kela K. Prevalence and etiology of nutritional anemia among school children of Urban Slums. Indian journal of medical research, 2003: 118: PP. 167- 171.
- United Nations children’s Fund (UNICEF). Prevalence and control of nutritional anemia (2003).
- Bermejo F, Garcia-Lopez S..A guide to diagnosis of iron deficiency anemia in digestive diseases. World journal of gastroenterology, 2009; 15(37). 4639.
- Greer J. P. Wintrob’s clinical haematology. 11th edition. London: Lippincott Williams and Wilkins, 2003: 794.
- World Health Organization (WHO). Iron deficiency anaemia; assessment, prevention and control. NHD/01.3 (2001).
- Abdelrahman EG, Gasim GA, Musa IR, ElbashirLM and Adam I. Red blood cell distribution width and iron deficiency anemia among pregnant Sudanese women. Diagnostic Pathology, 2012, 7:168.
- Asma MZ. A status of iron deficiency anemia among Sudanese pregnant women referred to Khartoum teaching hospital. MSc thesis, college of medical laboratory science. Sudan university of science and technology. 2012.
- Payandeh M, Rahimi Z, Zare ME, Kansestani AN, Gohardehi F, Hashemian AH. Prevalence of Anemia and Hemoglobinopathies in the Hematologic Clinics of the Kermanshah Province, Western Iran. International Journal of Hematology- Oncology and Stem Cell Research. 2014. 93(3):158-164.
- Lee JO, Lee JH, Ahn S, Kim JW, Chang H, Kim YJ, Lee KW, Kim JH, Bang SM, Lee JS. Prevalence and risk factors for iron deficiency anemia in the korean population: results of the fifth KoreaNational Health and Nutrition Examination Survey. J Korean Med Sci. 2014 Feb;29(2):224-9.
- Rohner F. Woodruff BA, Aaron GJ, Yakes EA, Lebanan MA, Rayco-Solon P, Saniel OP.Infant and young child feeding practices in urban Philippines and their association with stunting, anemia, and deficiencies of iron and vitamin A. Food and nutrition Bull, 2013; 34(2): PP. 73-81.
- Gongora D. G. Nutritional causes of anemia in Mexican children under 5 years: results from the 2006 National Health and Nutrition survey. SaludPaplica Mexico. 2012. 54(2):108-115.
- Lands R. H. Anemia in the elderly. Clinical Geriatrics, 2009;17(8):25-28.
- Alexandra M. Harrington, MD, MT(ASCP), Patrick C.J. Ward, MB, BCh, Steven H. Kroft, MD. Iron Deficiency Anemia, Beta-Thalassemia Minor, and Anemia of Chronic Disease: A Morphologic Reappraisal. Am J ClinPathol. 2008;129(3):466-471.
- Viswanath D, Hegde R, Murthy V, Nagashree S, Shah R. Red cell distribution width in the diagnosis of iron deficiency anemia. Indian J Pediatr. 2001. 68(12):1117-9.



