
Clinical Medicine Journal, Vol. 1, No. 1, April 2015 Publish Date: Apr. 2, 2015 Pages: 6-12
The Effect of Omega-3 on Health-Related Quality of Life in Individuals with Spinal Cord Injury: A Double-Blinded Randomized Clinical Trial
Hadis Sabour*, Sahar Latifi, Zahra Soltani, Abbas Norouzi Javidan, Mohammad Reza Hadian, Vahid Rafiei Manesh, Seyed-Hassan Emami Razavi, Seyed-Mohammad Ghodsi
Brain and Spinal Cord Injury Research Center, Neuroscience Institute, Tehran University of Medical Sciences, Tehran, Iran
Abstract
Objectives: The beneficial influences of omega-3 polyunsaturated fatty acids (PUFAs) in improving health-related quality of life (HR-QoL) have been demonstrated in some neurological diseases. However, this effect has not yet been described in spinal cord injury (SCI). Here, the effects of Omega-3 PUFA on HR-QoL among individuals with SCI have been assessed. Methods: One hundred and ten participants were randomly assigned to treatment and control groups. Patients in treatment group received two MorDHA capsules daily (435mg of docosahexaenoic acid and 65mg of eicosapentaenoic acid). Two placebo capsules were administered in control group. HR-QoL was assessed using Short-Form healthy survey (SF-36) at the beginning of the trial and then after 14 months. Results: After drop outs, 54 and 50 participants remained in treatment and control groups, respectively. In treatment group, mean difference in scores of Physical Component Summary and Mental Component Summary were -0.91 and 3.59, respectively which did not differ compared with control group (P= 0.90 and 0.40, respectively). Total score was 91.35±7.11 at the beginning of the trial in the treatment group and was increased to 93.84 ±6.36 after 14 months. Similarly, Total scores were changed from 92.63±7.03 to 93.31±7.51 in control group (P= 0.46). No significant effect of omega-3 PUFAs on any domains of SF-36 questionnaire could be detected. Conclusion: Our study does not support the beneficial effects of omega-3 fatty acid in improvement of QoL among individuals with SCI which may be due to lack of existence of active inflammatory reactions in stable phase of SCI.
Keywords
Quality of Life, Omega-3 Fatty Acids, Spinal Cord Injury, Health Survey
Received: March 21, 2015
Accepted: March 30, 2015
Published online: April 2, 2015
@ 2015 The Authors. Published by American Institute of Science. This Open Access article is under the CC BY-NC license. http://creativecommons.org/licenses/by-nc/4.0/
1. Introduction
Loss of motor function which occurs after spinal cord injury (SCI) leads to decreased quality of life (QoL) among affected individuals.1 Secondary complications that occur frequently after SCI also contributed to reduced QoL in this population.2 Many investigations have shown that people with SCI have lower QoL in comparison with general population.3-5 Improving health-related quality of life (HR-QoL) is a major clinical objective 6,7 especially when the increased incidence of SCI in developing countries is considered 8. Developing strategies to improve QoL is essential because it has been demonstrated that QoL can be a good predictor of survival 15 years after spinal injury 9.
QoL is a difficult term to define 10 and it is mostly considered to be subjective self-perceived health status. Many instruments have been developed to measure QoL. The Short-Form (SF-36) questionnaire is a standard tool which evaluates QoL in two main domains of Physical Component Summary (PCS) and Mental Component Summary (MCS) 11 and is widely used to assess QoL among patients with SCI. There are various factors that affect Qol in persons with SCI. Many studies have discussed the effect of age, level of injury and time since injury on Qol 12,13 whereas some other researches have focused on environmental issues such as social life, finance and employment 14,15. Furthermore, there are also studies that have investigated the effect of additional medical complications such as neurogenic bowel problems, neurogenic bladder and pain on Qol among these people 16. However, there are limited studies that have examined various interventions to improve QoL.
Previously some studies have shown that omega-3 poly unsaturated fatty acids (PUFA) has potential anti-inflammatory and neuroprotective effects and may have positive therapeutic influence in neurological diseases 17-19. Oleñik et al. 20 reported that omega-3 dietary supplement improves HR-QoL in both domains of MCS and PCS in patients with meibomian gland dysfunction. Similarly, Dashti-Khavidaki et al. 21 showed significant increased scores of physical and mental component summaries with consumption of omega-3 fatty acids in hemodialysis patients. Jelinek et al. 22 showed that taking omega-3 supplements or frequent consumption of fish in diet leads to significant improvement of QoL in all domains in patients with multiple sclerosis. Until now, no investigation has yet evaluated the effect of Omega-3 PUFAs on QoL in persons with SCI. By considering the positive influence of Omega-3 fatty acids on QoL which has been reported in other populations 20-22, we hypothesized whether similar outcomes can be found among individuals with SCI. The purpose of this study was to determine the effects of omega-3 PUFAs on HR-QoL assessed by SF-36 questionnaire in patients with SCI.
2. Materials and Methods
2.1. Participants
Patients with SCI who were referred to Brain and Spinal Injury Research Center (BASIR) between were invited to participate in this double-blinded randomized clinical trial (registration number: NCT01311375: 6 March 2011). Inclusion criteria were traumatic SCI and post-injury duration longer than 1 year. Exclusion criteria were as follows: pregnancy, lactation, amputation, non-traumatic SCI etiology, history of diabetes, cancer, endocrine disease, acute infection, and consumption of special medications such as glucocorticoid, hormones, thyroid hormones, anticonvulsive drugs, heparin, aluminum-containing antacids, lithium, omega-3 fatty acids or other nutrient supplements. Smokers and those who had regular consumption of alcohol or illegal drugs were excluded as well.
After obtaining informed written consent, 110 participants with SCI were enrolled and 55 patients were assigned to each of the treatment and control groups. Among them 104 participants completed the trial. Five patients in the control group and one patient in the treatment group did not complete the trial. The most common reasons for dropout were gastrointestinal complications and difficulty to follow routine visits’ schedules due to remote living location. Data were collected in BASIR from November 2010 to April 2012. The protocol was approved by the ethics committee of Tehran University of Medical Sciences (Approval number: 1421 at 18 July 2010).
2.2. Study Design
Randomization was performed using Permuted Balanced Block Randomization Method. After dropouts 54 and 50 participants remained in the treatment and control groups, respectively. Patients in the treatment group received two MorDHA® capsules (each capsule contains 465 mg of docosahexaenoic acid (DHA) and 63 mg of eicosapentaenoic acid (EPA)) per day and patients in the control group received two placebo capsules with similar size, taste and shape. The capsules were consumed with main daily meals (lunch and dinner). The duration of intervention was 14 months and assessment of QoL was performed once at the beginning of the trial and then after 14 months. The assessment of pill compliance was performed by using pill count method, which is based on a confidence relationship between patient and physician and was reported every 4 weeks 23. No dietary consults were given to patients and participants were encouraged to continue their routine diets and to exert no modifications to their dietary habits.
Omega-3 capsules were provided by Minami Nutrition Co. (Aartselaar, Belgium) and placebo capsules were supplied by Zahravi Pharmaceutical Co (Tehran, Iran). The recommended dose based on manufacturer guidelines of MorDHA® product is one capsule per day (each containing 465mg DHA and 63mg EPA). However, medical literatures have illustrated that a higher dose is required to obtain a significant effect in a specific medical disorder 24. After consulting with nutrition experts, we decided to prescribe two capsules of MorDHA® daily.
2.3. Clinical Measurements
Injury-related characteristics including completeness of injury, level of injury and American Spinal Injury Association (ASIA) Impairment Scale were measures. Completeness of injury was defined as either complete either complete (no preserved sensory or motor function) or incomplete (variable motor function preserved below the neurological level of injury). Descriptions of ASIA scales are as follows: ASIA-A indicates complete injury with no preserved motor or sensory function below the neurological level. ASIA-B describes incomplete injury in which only sensory function is preserved below the neurological level. ASIA-C illustrates preserved motor function in which more than half of key muscles below the neurological level have a muscle grade <3. ASIA-D indicates preserved motor function in which at least half of key muscles below the neurological level have a muscle grade of 3 or more 25.
2.4. Health-Related Quality of Life Assessment
HR-QoL was assessed using SF-36 questionnaire. This instrument is a standard measurement tool for assessment of QoL and has been used for a long time among people with SCI. The psychometric properties of the Iranian version of SF-36 questionnaire along with its validity and reliability are well documented 26. This measurement tool includes 36 items which assess QoL in eight domains: physical functioning (PF), role limitation due to physical problems (RP), bodily pain (BP), general health perceptions (GH), vitality (VT), social functioning (SF), role limitation due to emotional problems (RE) and mental health (MH). These scales provide two component summary scores: physical component summary (PCS) and mental component summary (MCS). Scores range from 0 to 100 and higher scores are representative of better QoL 27. PCS includes domains of physical functioning, role limitation due to physical problems, bodily pain and general health. MCS includes domains of vitality, social functioning, role limitation due to emotional problems and mental health.
2.5. Statistical Analysis
All statistical analysis was performed using SPSS ver. 21 software (IBM Corporation). The chi-square test (Fisher’s exact test) was used to compare categorical variables in univariate analysis. The comparison of SF-36 scores between groups was performed using One-way Analysis of Variance (ANOVA). Categorical data are reported using percentages and continuous quantitative values are reported by mean± standard deviation (SD). The mean differences between the scores at the beginning and at the end of the trial were measured and these mean differences were compared between treatment and control groups. Correlation analysis was used to evaluate the relationship between continuous variables. Age, time since injury, injury level and completeness, ASIA score and plegia type (tetraplegia vs. paraplegia) were considered as independent variables. P<0.05 was considered to be statistically significant.
3. Results
Fifty four participant with mean age of 51.15±13.43 years and 50 patients with mean age of 54.12± 11.76 years were included in the treatment and the control group, respectively. Time since injury was 8.96±5.44 in the treatment group and 9.56±7.20 in the placebo group. Age and time since injury did not differ between the two groups (P= 0.23 and 0.63, respectively). The majority of patients were men (16.7% (n: 19) females vs 74.6% (n: 85) males). Baseline characteristics of the participants are illustrated in table 1. The most common injury level was at thoracic sections (59.3% and 66% in the treatment and control groups, respectively). Most patients had complete SCI (74% in the treatment group and 76% in the control group). There was no significant difference in level and completeness of the injury between the two groups (P= 0.29 and 0.39, respectively). ASIA-A was the most frequent Impairment Scale in both groups and no difference in the distribution of ASIA scales was found between treatment and control groups (P= 0.65).
Table 1. Baseline characteristics in the participants in treatment and control groups
| Category | Treatment Group | Control Group | P-value | |||
| Number (percentage) | Mean (SD) | Number (percentage) | Mean (SD) | |||
| Gender | Men | 44 (81.5) | - | 41 (82.0) | - | 0.57 |
| Women | 10 (18.5) | - | 9 (18.0) | - | ||
| Level of the Injury | Cervical | 14 (25.9) | - | 7 (14.0) | - | 0.29 |
| Thoracic | 32 (59.3) | - | 33 (66.0) | - | ||
| Lumbar | 8 (14.8) | - | 10 (20.0) | - | ||
| Completeness of the injury | Complete | 40 (74.0) | - | 38 (76.0) | - | 0.39 |
| Incomplete | 14 (26.0) | - | 12 (24.0) | - | ||
| Plegia | Paraplegia | 44 (81.5) | - | 47 (94.0) | - | 0.05 |
| Tetraplegia | 10 (18.5) | - | 3 (6.0) | - | ||
| ASIA Scale | A | 40 (74.0) | 38 (76.0) | 0.65 | ||
| B | 7 (13.0) | 5 (10.0) | ||||
| C | 1 (1.9) | 3 (6.0) | ||||
| D | 6 (11.1) | 4 (8.0) | ||||
| Age (years) | 51.15 (13.43) | 54.12 (11.76) | 0.23 | |||
| Time since injury (years) | 8.96 (5.44) | 9.56 (7.20) | 0.63 | |||
ASIA: American Spinal Injury Association, SD: Standard Deviation
Table 2. Mean scores in domains of sf-36 questionnaire in treatment and control group and the mean differences after 14 months of omega-3 fatty acid administration
| Category | Treatment group (n: 54) | Control group | P-value | ||||
| At the beginning | After 14 months | Mean Difference | At the beginning | After 14 months | Mean Difference | ||
| Mean (SD) | Mean | Mean (SD) | Mean | ||||
| PF | 15.69 (4.53) | 16.00 (3.84) | 0.80 | 15.63 (4.31) | 16.49 (4.02) | 0.73 | 0.98 |
| RP | 6.88 (1.60) | 7.59 (1.15) | 0.83 | 6.82 (1.59) | 7.41 (1.22) | 0.50 | 0.37 |
| BP | 5.04 (2.59) | 3.55 (1.90) | -1.52 | 4.27 (2.21) | 3.46 (1.21) | -0.79 | 0.09 |
| GH | 18.24 (2.70) | 17.51 (2.34) | -0.98 | 18.30 (3.41) | 17.18 (2.16) | -1.06 | 0.92 |
| VT | 15.00 (2.13) | 17.00 (1.98) | 2.15 | 15.38 (2.69) | 16.00 (2.22) | 1.14 | 0.09 |
| SF | 6.00 (0.93) | 6.00 (0.74) | 0.02 | 5.88 (0.69) | 5.95 (0.39) | 0.11 | 0.74 |
| RE | 5.06 (1.40) | 5.29 (1.17) | 0.33 | 5.04 (1.25) | 5.97 (3.44) | 0.84 | 0.36 |
| MH | 19.52 (1.93) | 20.82 (2.15) | 1.21 | 20.28 (2.14) | 20.85 (2.23) | 0.60 | 0.26 |
| PCS | 45.68 (5.27) | 44.72 (4.06) | -0.91 | 45.20 (6.08) | 44.54 (4.80) | -0.76 | 0.90 |
| MCS | 45.69 (3.72) | 49.12 (4.14) | 3.59 | 46.67 (4.39) | 48.77 (5.72) | 2.67 | 0.40 |
| Total | 91.35 (7.11) | 93.84 (6.36) | 2.63 | 92.63 (7.03) | 93.31 (7.51) | 1.48 | 0.46 |
BP: Bodily pain, GH: General Health, MH: Mental Health, PF: Physical functioning, RE: Role limitation due to emotional problems, RP: Role limitation due to physical problems, SF: Social functioning, VT: Vitality
Table 3. The relationships between injury-related characteristics and total scores in SF-36 health survey in treatment and control groups. (The reported values are P-values calculated by One-way Analysis of Variance (ANOVA)).
| Category | Treatment Group | Control Group | ||
| At the beginning | After 14 months | At the beginning | After 14 months | |
| Level of the injury | 0.02* | 0.04* | 0.019* | 0.017* |
| Completeness of the injury | 0.64 | 0.45 | 0.92 | 0.59 |
| ASIA scale | 0.45 | 0.50 | 0.10 | 0.90 |
| Plegia type | 0.86 | 0.68 | 0.21 | 0.97 |
* Statistically significant at the level of P<0.05
ASIA: American Spinal Injury Association
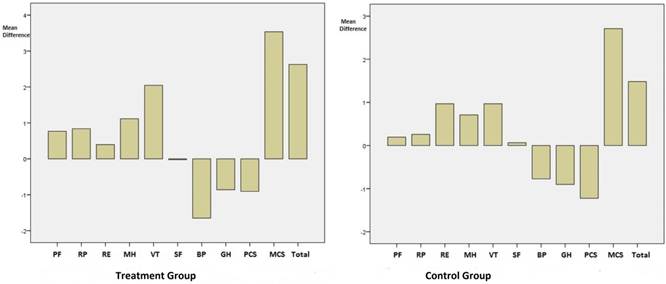
Figure 1. Changes in the scores of SF-36 domains after 14 months in treatment and control groups
The mean scores of PCS and MCS at the beginning of the trial in treatment group were 45.68±5.27 and 45.69±3.72, respectively. These scores had insignificant change after 14 months of administration of omega-3 PUFAs (44.72± 4.06 and 49.12±4.14 for PCS and MCS, respectively). In treatment group mean difference in PCS and MCS scores were -0.91 and 3.59, respectively and in control group these measures were -0.76 and 1.48. No significant difference in the amount of change in PCS and MCS scores could be found between the two groups (P= 0.90 and 0.40, respectively) which illustrate the insignificant effect of omega-3 fatty acid administration on these domains. Similarly, total scores at the beginning of the trial were 91.35±7.11 and 92.63± 7.03 in treatment and control groups, respectively and these measures were changed to 93.84±6.36 and 93.31±7.51 at the end of the trial. The mean difference in total score was 2.63 in treatment group which did not differ significantly with control group (mean difference: 1.48; P= 0.46) (table 2).
Although the changes in the mean scores of all domains were insignificant after 14 months of administration of omega-3 PUFA, the trend in the domains of bodily pain and general health was toward reduction in both groups (figure 1). Since increased scores of MCS as well as total scores were observed in both groups, these changes cannot be assigned to omega-3 PUFA effect.
Among injury-related characteristics, only level of injury was a determinant of QoL in both groups at the beginning and at the end of the trial. Total scores at the beginning and after 14 months were significantly higher among patients with injury at lumbar level. (P= 0.02 and 0.04, respectively in treatment group, P= 0.019 and 0.017, respectively in control group) (table 3). Completeness of the injury, ASIA scale and plegia type (tetraplegia vs. paraplegia) were not associated with HR-QoL.
4. Discussion
The neuroprotective effect of omega-3 fatty acids have been previously illustrated in multiple sclerosis (MS) 28, 29. Many investigations have supported the effect of omega-3 PUFAs in induction of neuro-recovery 30, 31. The anti-inflammatory and neuroprotetive effects of omega-3 PUFA have led to increased QoL in patients with meibomian gland dysfunction 20, MS 22 and hemodialysis patients 21. However, the effects of omega-3 PUFA on QoL in spinal cord injury have not yet been described. In this study, the effects of 14 months administration of omega-3 PUFA was insignificant in all domains of HR-QoL assessed by SF-36 questionnaire. One reason is that we administered the omega-3 supplements in the stable phase of SCI. The effects of omega-3 fatty acids are mediated through their anti-inflammatory and anti-oxidative influences which are mostly effective in the acute phase of the injury, in which the inflammatory reactions are at their peak level 32. Therefore, we can conclude that the insignificant effects of omega-3 PUFAs in stable chronic SCI is due to low levels of inflammatory cytokines among these patients. A continuous degenerative and inflammatory process can be observed in MS which enables omega-3 fatty acids to be more effective than in SCI. In the present investigation only patients in stable phase of SCI with post injury duration longer than 1 year were recruited. One reason that we did not investigate patients in acute phase of SCI was that the majority of these patients are hospitalized which affects their subjective self-perceive of health. Moreover many of these patients may experience denial or depressive phases 33 which have bias effects in assessment of QoL. Furthermore, the increased QoL through time in acute phase can be assigned to rehabilitation programs and management of injury-related complications rather than omega-3 administration. Since many of these rehabilitations and medical programs are essential for patients, the designing of clinical trials in the acute phase of SCI mostly encounters difficulties. Previous literatures has supported the fact that a state of chronic inflammation occurs after SCI 34, 35 and this steady inflammation even explained higher risk of atherogenic events in these patients 35. However, even by considering the existence of chronic inflammatory processes in SCI, our results have shown that omega-3 supplements are not effective agents in improving QoL among affected individuals.
The beneficial effect of omega-3 PUFAs in improvement of QoL in MS was medicated through decreased rate of disease relapse 22. The expected improved QoL in SCI is assumed to be correlated with increased independency and better neurorehabilitation outcomes. However, our previous report 36 showed no effect of omega-3 PUFAs on neurorehabilitation and scores of dependency among affected individuals which may explain the insignificant effect of omega-3 supplements on QoL in this study.
In the present study, scores in mental component summary as well as total scores raised through time in both groups whereas the trend in physical component summary, bodily pain and general health was toward reduction. Since these changes have occurred in both groups of treatment and control, they cannot be assigned to administration of omega-3 supplements. Further investigations should be performed to identify the factors that affect QoL among individuals with SCI through time.
Level of injury was the only major determinant of QoL among injury-related characteristics and patients with injury at lumbar levels at significantly better QoL in treatment and control groups. Since this association was observed in both groups and existed from the beginning of the trial it cannot be assigned to omega-3 supplement prescription and it also can be concluded that these associations are not affected by omega-3 fatty acids since they remained being significant until the end of the trial. More severe loss of function which occurs in individuals with higher injury level may contribute to lower QoL among these patients 37. Unlike the level of the injury, completeness of injury was not related to QoL. There are conflicting results on the effect of injury completeness on QoL. Some investigations have shown better QoL among patients with incomplete injury 37, 38 and others, including our study, have demonstrated no effect of completeness of the injury on HR-QoL 39, 40. There are similar conflicting reports on the effect of plegia type (tetraplegia vs. paraplegia)on QoL. Previously, Lin et al. 41 reported that tetrapegics have poorer QoL in comparison with people with paraplegia. However, in line with some other studies 42, 43, no effect of plegia type on HR-QoL could be detected in our study. Ebrahimzadeh et al. 43 described that the insignificant difference in QoL between people with tetraplegia vs. paraplegia is due to the existence of accessible facilities and recreational programs for patients with tetraplegia which improves their degree of independency. However, by considering the various factors that affects QoL including educational level, employment status, income, social activities and familial support 44, further investigations with control for these confounders are required to clarify the effects of completeness of the injury and plegia type on QoL.
5. Conclusion
While many investigations have supported the beneficial effects of omega-3 fatty acid in improving QoL in patients with neurological diseases such as MS, the influence of these therapeutic agents on QoL in SCI is insignificant which may be due to lack of existence of active inflammatory reactions in stable phase of SCI. Our study does not support the beneficial effects of omega-3 fatty acid in improvement of QoL among individuals with SCI.
References
- Boswell B, Dawson M, Heininger E. Quality of life as defined by adults with spinal cord injuries. J Rehabil. 1998;64:27–32.
- Cardenas DD, Hoffman JM, Kirshblum S, McKinley W. Etiology and incidence of rehospitalization after traumatic spinal cord injury: a multicenter analysis. Arch Phys Med Rehabil. 2004;85:1757–1763.
- Post M, VanDijk A, Asbeck F, Schrijvers A. Life satisfaction of persons with SCI compared to a population group. Scand J Rehabil Med. 1998;30:23–30.
- Anderson CJ, Vogel LC, Chlan KM, Betz RR, McDonald CM.Depression in adults who sustained spinal cord injuries as children or adolescents. J Spinal Cord Med. 2007;30(Suppl 1):S76–S82.
- Dijkers MP. Individualization in quality of life measurement: instruments and approaches. Arch Phys Med Rehabil. 2003;84:S3–S14.
- Hammell KW. Quality of life after spinal cord injury: a meta-synthesis of qualitative findings. Spinal Cord. 2007;45:124-139.
- May LA, Warren S. Measuring quality of life of persons with spinal cord injury: external and structural validity. Spinal Cord. 2002; 40(7):341–350.
- Rahimi-Movaghar V, Sayyah MK, Akbari H, Khorramirouz R, Rasouli MR, Moradi-Lakeh M, et al. Epidemiology of traumatic spinal cord injury in developing countries: a systematic review. Neuroepidemiology. 2013;41(2):65–85.
- Krause JS, Kjorsvig JM. Mortality after spinal cord injury: a four year prospective study. Arch Phys Med Rehabil. 1992;73:558–563.
- Moons P, Van Deyk K, Budts W, De Geest S. Caliber of quality-of-life assessments in congenital heart disease: a plea for more conceptual and methodological rigor. Arch Pediatr Adolesc Med.2004; 158(11):1062–1069.
- Ware JE, Sherbourne CD. The MOS 36-item short-form health survey (SF- 36). I. Conceptual framework and item selection. Med Care. 1992;30:473-483.
- Kennedy P, Rogers B. Reported quality of life of people with spinal cord injuries: a longitudinal analysis of the first 6 months post-discharge. Spinal Cord. 2000;38:498–503.
- Putzke JD, Richards JS, Hicken BL, DeVivo MJ. Predictors of life satisfaction: a spinal cord injury cohort study. Arch Phys Med Rehabil. 2002;83:555–561.
- Lund ML, Nordlund A, Nygard L, Lexell J, Bernspang B. Perceptions of participation and predictors of perceived problems with participation in persons with spinal cord injury. J Rehabil Med. 2005;37:3–8.
- Elfström ML, Rydén A, Kreuter M, Taft C, Sullivan M. Relations between coping strategies and health-related quality of life in patients with spinal cord lesion. J Rehabil Med. 2005;37:9–16.
- Liu CW, Huang CC, Yang YH, Chen SC, Weng MC, Huang MH. Relationship between neurogenic bowel dysfunction and health-related quality of life in persons with spinal cord injury. J Rehabil Med. 2009;41(1):35-40.
- Lauritzen I, Blondeau N, Heurteaux C, Widmann C, Romey G, Lazdunski M. Polyunsaturated fatty acids are potent neuroprotectors. EMBO J 2000;19(8):1784–93.
- Emsley R, Oosthuizen P, van Rensburg SJ. Clinical potential o omega-3 fatty acids in the treatment of schizophrenia. CNS Drugs. 2003;17(15):1081–91.
- Endres S, von Schacky C. n-3 polyunsaturated fatty acids and human cytokine synthesis. Curr Opin Lipidol. 1996;7(1):48–52.
- Oleñik A, Mahillo-Fernández I, Alejandre-Alba N, Fernández-Sanz G, Pérez MA, Luxan S, et al. Benefits of omega-3 fatty acid dietary supplementation on health-related quality of life in patients with meibomian gland dysfunction. Clin Ophthalmol. 2014;8:831-6.
- Dashti-Khavidaki S, Gharekhani A, Khatami MR, Miri ES, Khalili H, Razeghi E, et al. Effects of omega-3 fatty acids on depression and quality of life in maintenance hemodialysis patients. Am J Ther. 2014;21(4):275-87.
- Jelinek GA, Hadgkiss EJ, Weiland TJ, Pereira NG, Marck CH, van der Meer DM.Association of fish consumption andΩ3 supplementation with quality of life, disability and disease activity in an international cohort of people with multiple sclerosis. Int J Neurosci. 2013;123(11):792-800.
- Sabour H, Javidan AN, Latifi S, Shidfar F, Heshmat R, Emami Razavi SH, et al. Omega-3 fatty acids' effect on leptin and adiponectin concentrations in patients with spinal cord injury: A double-blinded randomized clinical trial. J Spinal Cord Med. 2014.
- Omega-3 fatty acids, fish oil, alpha-linolenic acid. Available at:http://www.mayoclinic.org/drugs-supplements/omega-3-fatty-acids-fish-oil-alpha-linolenic-acid/dosing/hrb-20059372.
- Kirshblum SC, Burns SP, Biering-Sørensen F, DonovanW, Graves DE, Jha A, et al. International standards for neurological classification of spinal cord injury (revised 2011). J Spinal Cord Med. 2011;34(6):535–46.
- Montazeri A, Goshtasebi A, Vahdaninia M, Gandek B. The Short Form Health Survey (SF-36): translation and validation study of the Iranian version. Qual Life Res. 2005;14: 875–882.
- Ware JE, Kosinski M, Keller SK.SF-36 Physical and Mental Health Summary Scales: A User’s Manual Boston, MA. The Health Institute 1994.
- Esparza ML, Sasaki S, Kesteloot H. Nutrition, latitude, and multiple sclerosis mortality: an ecologic study. Am J Epidemiol 1995;142(7):733–7.
- Gallai V, Sarchielli P, Trequattrini A, Franceschini M, Floridi A, Firenze C. et al. Cytokine secretion and eicosanoid production in the peripheral blood mononuclear cells of MS patients undergoing dietary supplementation with n-3 polyunsaturated fatty acids. J Neuroimmunol 1995;56:143–53.
- King VR, Huang WL, Dyall SC, Curran OE, Priestley JV, Michael-Titus AT. Omega-3 fatty acids improve recovery, whereas omega-6 fatty acids worsen outcome, after spinal cord injury in the adult rat. J Neurosci. 2006;26:4672–4680.
- Lang-Lazdunski L, Blondeau N, Jarretou G, Lazdunski M, Heurteaux C. Linolenic acid prevents neuronal cell death and paraplegia after transient spinal cord ischemia in rats. J Vasc Surg. 2003; 38:564–575.
- Mori TA, Beilin LJ. Omega-3 fatty acids and inflammation. Curr Atheroscler Rep. 2004;6:461–467.
- Hancock KM, Craig AR, Dickson HG, Chang E, Martin J. Anxiety and depression over the first year of spinal cord injury: a longitudinal study. Paraplegia. 1993;31(6):349-57.
- da Silva Alves E, de Aquino Lemos V, Ruiz da Silva F, Lira FS, Dos Santos RV, Rosa JP. et al.Low-grade inflammation and spinal cord injury: exercise as therapy? Mediators Inflamm 2013; 2013: 971841.
- Wang TD, Wang YH, Huang TS, Su TC, Pan SL, Chen SY. Circulating levels of markers of inflammation and endothelial activation are increased in men with chronic spinal cord injury. J Formos Med Assoc. 2007;106: 919–928.
- Norouzi Javidan A, Sabour H, Latifi S, Abrishamkar M, Soltani Z, Shidfar F, et al. Does consumption of polyunsaturated fatty acids influence on neurorehabilitation in traumatic spinal cord-injured individuals? A double-blinded clinical trial. Spinal Cord. 2014;52(5):378-82.
- Jain NB, Sullivan M, Kazis LE, Tun CG, Garshick E. Factors associated with health-related quality of life in chronic spinal cord injury. Am J Phys Med Rehabil. 2007;86(5):387-96
- Hu Y, Mak JN, Wong YW, Leong JC, Luk KD. Quality of life of traumatic spinal cord injured patients in Hong Kong. J Rehabil Med. 2008;40:126-131.
- Fuhrer MJ, Rintala DH, Hart KA, Clearman R, Young ME. Relationship of life satisfaction to impairment, disability, and handicap among persons with spinal cord injury living in the community. Arch Phys Med Rehabil. 1992;73:552–7.
- Manns PJ, Chad KE. Determining the relation between quality of life, handicap, fitness, and physical activity for persons with spinal cord injury. Arch Phys Med Rehabil. 1999;80:1566–71.
- Lin KH, Chuang CC, Kao MJ, Lien IN, Tsauo JY.Quality of life of spinal cord injured patients in Taiwan: a subgroup study. Spinal Cord. 1997;35(12):841-9.
- Lidal IB, Veenstra M, Hjeltnes N, Biering-Sorensen F. Health-related quality of life in person with long-standing spinal cord injury. Spinal Cord. 2008;46:710-715.
- Ebrahimzadeh MH, Soltani-Moghaddas SH, Birjandinejad A, Omidi-Kashani F, Bozorgnia S. Quality of life among veterans with chronic spinal cord injury and related variables. Arch Trauma Res. 2014;3(2):e17917.
- Clayton KS, Chubon RA. Factors associated with the quality of life of long-term spinal cord injured persons. Arch Phys Med Rehabil. 1994;75(6):633-8.



