
American Journal of Economics, Finance and Management, Vol. 1, No. 3, June 2015 Publish Date: Apr. 10, 2015 Pages: 97-101
Trend of Healthcare Expenditures in Bangladesh over Last Decades
Rashidul Alam Mahumud*, Marufa Sultana, Abdur Razzaque Sarker
Health Economics and Financing Research Group, Centre for Equity and Health System, International Centre for Diarrhoeal Disease Research, Bangladesh (icddr,b), Dhaka, Bangladesh
Abstract
Background: The rapid growth of healthcare expenditure has become a great concern for both for private and public viewpoint. Healthcare expenditures comprise a great share of government budget and expenditures and it is the key issue that dominates health policy and its indicators. Objective: The objective of the study is to investigate the trend of determinants of healthcare expenditure after controlling for country-specific economic conditions and comparing between public and private health care spending across the country. Methods: The study extracted cross-sectional and annual time series data from the World Development Indicators over 1995 to 2010 for Bangladesh context. Simple regression analysis and t-test were performed to identify the trend of healthcare expenditure and compared between the private and public healthcare expenditure. Correlation matrix was used to examine the interrelationship among the study variables. Results: Private healthcare expenditure in Bangladesh has been increasing although the public healthcare expenditure has been declining over the period. In correlation matrix results showed that private healthcare expenditure as a share of GDP and GDP growth had a strong positive relationship with the total healthcare expenditure and healthcare expenditure per capita. The study also investigated that there was a significant reverse relationship between public and private sector healthcare expenditure. Conclusion: The study emerge to establish effective public-private partnerships in developing the health sector which can help the policymakers to make long term decisions to improve population health status.
Keywords
Health Care Expenditure, GDP, Private and Public Sector and Trend Analysis
Received: March 23, 2015
Accepted: April 9, 2015
Published online: April 10, 2015
@ 2015 The Authors. Published by American Institute of Science. This Open Access article is under the CC BY-NC license. http://creativecommons.org/licenses/by-nc/4.0/
1. Background
Bangladesh has achieved many notable improvements in economic, social and health development over the past decades such as reducing poverty, improving life expectancy, maternal health, fertility control, child mortality. Through, improving health indicators, healthcare expenditures also comprise a great share of government budget and became a key issues that dominates health policy and its indicators [1-2]. The total healthcare expenditure includes spending by both public and private sources like medical goods and services, prevention programs, and administration [3]. The public healthcare expenditures are usually financed through social security contributions, various forms of taxation to various branches of government and from external sources [4]. On the contrary, the private healthcare expenditures encompass private insurance premiums and prepaid schemes, mandated enterprise health expenditure, expenditure on health through non-profit health services and direct of pocket expenditure on health goods, which includes co-payments as well as direct payments by uninsured individuals [5]. A previous study found that adequate and efficient healthcare spending widely considered as expected in the improvement of health status [6-7]. However, it was already proven that the demand for healthcare services was a leading factor to increase in healthcare expenditure in many countries. An earlier studies conducted using panel data found that government healthcare expenditure followed different paths and its growth was different in developing countries at different levels of economic development [8-9]. The purpose of the study was, therefore, three-fold, first was to investigate the trend of determinants of healthcare spending after controlling for country-specific economic conditions. Secondly, a differential analysis of public and private health care spending was performed. Thirdly, find out the interrelationship among the determinants of health care expenditure.
2. Methods
The study conducted through the cross-sectional and annual time series data from 1995 to 2010 for Bangladesh. The data used in the empirical analysis were sourced from World Development Indicators (WDI) of World Bank [10]. The present study used variables related to health care expenditure such as GDP growth (annual %), GDP per capita in PPP (constant 2005 international $), healthcare expenditure per capita in PPP (constant2005 int.$), private healthcare expenditure(% of GDP), public healthcare expenditure(% of GDP), total healthcare expenditure(% of GDP), public healthcare expenditure(% of government expenditure), and public healthcare expenditure(% of total health expenditure). For comparing the healthcare expenditure for public and private sector, these data has been analyzed through the various statistical measures like descriptive statistics, simple regression analysis and trend analysis. Correlation matrix was employed to determine inter relationship among the determinants of health expenditure. T-test was employed to investigate the significant difference in change of growth between the public and private sector in case of healthcare expenditure in Bangladesh. All statistical analyses were accomplished through the statistical software STATA-13.
3. Results
3.1. Descriptive Statistics
Table 1 showed the descriptive statistics of the determinants of healthcare expenditure. Average, standard deviation (SD), 95% CI for mean and number of observations (on the basis of which the statistics were calculated) were presented. GDP growth and GDP per capita were 5.58%± 0.671% & US$1095.25 ± US$ 209.303, respectively. Also, per capita healthcare expenditure was US$ 12.68 ± US$4.61. Public and private healthcare expenditure as a share of GDP were 1.99% ± 0.265% and 1.17% ± 0.063% respectively. Total healthcare expenditure as a share of GDP was 3.16% ± 0.288%. Furthermore, public healthcare expenditure as a share of government expenditure on health was 8.03 % ± 0.723%.
Table 1. The Results of Descriptive Statistics.
| Variables | Mean | SD | 95 % CI for Mean | |
| Lower Bound | Upper Bound | |||
| GDP Growth (%) | 5.58 | 0.67 | 5.22 | 5.93 |
| GDP Per Capita (US$) | 1095.25 | 209.30 | 983.72 | 1206.78 |
| Healthcare expenditure per capita (US$) | 32.32 | 13.27 | 25.25 | 39.39 |
| Private Healthcare expenditure(% of GDP) | 1.99 | 0.27 | 1.85 | 2.13 |
| Public healthcare expenditure(% of GDP) | 1.17 | 0.063 | 1.14 | 1.2 |
| Total healthcare expenditure(% of GDP) | 3.16 | 0.29 | 3.01 | 3.31 |
| Public health expenditure (% of Government expenditure) | 8.03 | 0.72 | 7.64 | 8.41 |
| Public healthcare expenditure (% of Total health expenditure) | 37.16 | 0.083 | 35.51 | 38.8 |
3.2. Trend Analysis
Figure 1 showed the trend of determinants of health expenditure. Public healthcare expenditure as a share of GDP was stabilized from 1995 but private healthcare expenditure was increasing from the early 1997s. The overall total healthcare expenditure as share of GDP had rising tendency though it was fallen from 3.46% to 2.73% in between 1996 to 1998. However, public healthcare expenditure as a share of total government expenditure was slightly turned down (Figure 1).
Figure 2 showed per capita healthcare expenditure as a share of total healthcare expenditure as increased more rapidly since 1997s though the public healthcare expenditure as a share of total healthcare expenditure had decreasing.
3.3. Simple Regression Analysis
Table 2 demonstrated the coefficients of regression analysis. GDP growth and GDP per capita increased yearly by 0.0993% and US$ 43.213 respectively (P<0.001). However, public healthcare expenditure as a share of GDP, public healthcare expenditure as a share of government expenditure and public healthcare expenditure as a share of total healthcare expenditure decreased by 0.004%, 0.1061% and 0.4476% respectively.
Table 3 showed the difference private and public expenditure on health as share of GDP. Result exhibited that significant difference exits between private and public expenditure (P<0.000).
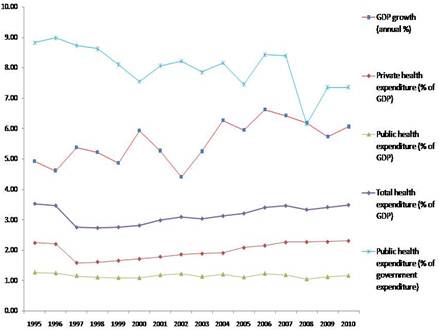
Figure 1. Trend of GDP growth, public, private and total healthcare expenditure as a share of GDP, public healthcare expenditure as a share of government expenditure.
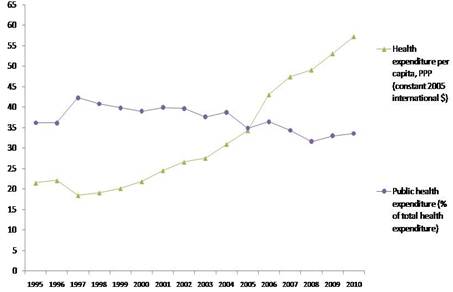
Figure 2. Trend of per capita healthcare expenditure and public healthcare expenditure as a share of total health expenditure.
Table 2. The results of simple regression analysis.
| Variables | Model | Coefficient | R2(%) |
| GDP growth (annual %) | GDPG = 4.73 + 0.09 year | 0.09*** | 49.52 |
| GDP per capita | GDP_PC = 727.94 + 43.21 year | 43.21** | 96.62 |
| Healthcare expenditure per capita(HEPC) | HEPC = 10.16 + 2.61year | 2.61*** | 87.47 |
| Private healthcare expenditure (% of GDP) | Pvt_GDP = 1.73 + 0.031 year | 0.031*** | 30.92 |
| Public healthcare expenditure (% of GDP) | Pub_GDP = 1.20 – 0.004 year | -0.004* | 8.95 |
| Total healthcare expenditure (% of GDP) | Total_GDP = 2.93 + 0.027 year | 0.027** | 19.93 |
| Public healthcare expenditure (% of government expenditure) | Pub_GE = 8.93 – 0.11 year | -0.106* | 48.88 |
| Public health expenditure (% of total health expenditure) | Pub_THE = 40.96 - 0.45year | -0.45*** | 47.77 |
NOTE:***, ** and * denoted 1%, 5% and 10% level of significance
Table 3. The results of the t-test for the public and private healthcare expenditure as a share of GDP.
| Variable | N | Mean | Std. Dev. | 95% CI of Mean | P-value | |
| Lower Bound | Upper Bound | |||||
| Public healthcare expenditure (% of GDP) | 16 | 1.17 | 0.06 | 1.14 | 1.2 | 0.05 |
| Private healthcare expenditure (%of GDP) | 16 | 1.99 | 0.27 | 1.85 | 2.14 | |
NOTE: * denoted at 5 % level of significance
3.4. Correlation Matrix
Table 4 demonstrated the coefficients of correlation matrix for determinants of healthcare expenditure. Private healthcare expenditure as a share of GDP showed strong positive relationship (r = 0.98) with total healthcare expenditure as a share of GDP (p<0.00). However, healthcare expenditure per capita had positive relationship with GDP growth (r=0.67), private (r=0.76) and total (r=0.67) healthcare expenditure (P<0.01).
Table 4. The Result of the correlation matrix among the determinant of health expenditures in Bangladesh.
| Variables | Healthcare expenditure per capita | GDP growth | Private healthcare expenditure (% of GDP) | Public healthcare expenditure (% of GDP) | Total healthcare expenditure (% of GDP) | Private healthcare expenditure (% of THE) |
| Healthcare expenditure per capita | 1 | |||||
| GDP growth | 0.67*** | 1 | ||||
| Private healthcare expenditure (% of GDP) | 0.76*** | 0.37 | 1 | |||
| Public healthcare expenditure (% of GDP) | -0.15 | -0.23 | 0.26 | 1 | ||
| Total health expenditure ( % of GDP) | 0.67*** | 0.29 | 0.98 | -0.45* | 1 | |
| Private health expenditure (% of THE) | 0.38*** | -0.47* | 0.23 | 0.12 | 0.23*** | 1 |
NOTE: *** and * denoted 1% and 10% level of significance
4. Discussion
This study investigated the trend of determinants of healthcare expenditure and also established the interrelationship among those determinants. Study found that total healthcare expenditure and private healthcare expenditure as a share of GDP had been increasing since 1997s, but public healthcare expenditure remained stable since 1995. Healthcare expenditure per capita increased more rapidly from 1997s where private healthcare expenditure was highly correlated with the total health expenditure. In this study, the share of public healthcare expenditure had downward movement after 1996s. On the other hand, private healthcare expenditure and GDP growth had significant relationship with the total healthcare expenditure and per capita health expenditure. Although the other study demonstrated that the private health expenditures had significant negative relationship with the health expenditures [2]. However, it may completely depends on some key issues such as household decision maker, economic status, public funding on health, educational status, knowledge about skill healthcare provider, quality of health services and so on.
In general, private healthcare expenditure was increased because the private sectors made informed choices about the type of services they wish to purchase. In making this choice, they purchased private health services either directly or indirectly via private health insurance[11]. Another observation was that private healthcare expenditure increased in response to a shortfall of public funding for a given level of demand or need in the community. The longer waiting time for some services may force people to skip queues by purchasing services either directly or indirectly through private health insurance. Different private funding mechanisms might also be explained by a belief held by decision-makers that a move to allocate health resources by user charges and privatization may effectively control demand, prices and the supply of services. Although the average percentage of household income devoted to private expenditure on health increased over the period of time in Bangladesh, there was no regressive change in the payments. This indicated that the policies might work initially to minimize the impact of these payments on low-income households. Attempts to change the outline of private healthcare expenditure to low-income households requires a review of society’s commitment to both health, age, sex and income equity [12]. Progress towards the achievement of both was most likely to be accomplished through macroeconomic growth and stability. The findings of the study are expected to be used for providing and developing health facilities and improving health system operations specially in public health expenditure. This was similar with findings of other studies that healthcare expenditure is an important determinant of health outcomes both at the individual and national levels [13-14]. It should be noted that the findings of the current study can provides evidence in support of increasing health care expenditure, which may only be a necessity but not sufficient condition for achieving progress in terms of population health which may depend on the effective and efficient allocation of such resources.
One limitation of this study was the selection of specific variables of interest where most of the healthcare expenditure determinants for Bangladesh did not have enough time series observation which would have improved a panel data study. Published data were not available on some of the key variables of interests that may affect healthcare expenditure determinants.
5. Conclusions
The study found that the private healthcare expenditure in Bangladesh is increasing although the public healthcare expenditure still declining over the same period. Establishment of effective public-private partnerships in developing health sector can help the policymakers to make long term decisions to improve population health status.
Acknowledgements
icddr,b is thankful to the Governments of Australia, Bangladesh, Canada, Sweden and the UK for providing core/unrestricted support. The authors would also like to the thank health economics and financing research groups for their comments on an earlier draft of the manuscript.
References
- S.Roy. Determinants of healthcare expenditure on human capital and economic growth in Bangladesh: a longitudinal data analysis from 1995-2010. Asian J Pharmaceut Res Health Care 2014; 6: 6–10.
- A. Samadi & R. Homaie. Determinants of Healthcare Expenditure in Economic Cooperation Organization (ECO) Countries: Evidence from Panel Cointegration Tests. International Journal of Health Policy and Management 2013;1: 63–68.
- OECD. OECD ilibrary, 2014.
- P. Poullier, K. Kawabata, & D. Savedoff. National health accounts: concepts, data source and methodology. Geneva, Switzerland: World Health Organization 2001.
- J. Novignon, S. Olakojo, & J Nonvignon. The effects of public and private health care expenditure on health status in sub-Saharan Africa: new evidence from panel data analysis. Health Economics Review 2012; 2: 22.
- J.C.Anyanwu, & A. Erhijakpor. Health Expenditures and Health Outcomes in Africa (Vol. 91) Tunisia, 2007.
- R.A. Mahumud, L.B. Rawal, G.Hossain, R.Hossain, N. Islam.Impact of Life Expectancy on Economics Growth and Health Care Expenditures: A Case of BangladeshUniversal Journal of Public Health 2013; 1:180-186.
- J.A.M. Khan&R. A. Mahumud. Is healthcare a ‘Necessity’ or ‘Luxury’? an empirical evidence from public and private sector analyses of South-East Asian countries? Health Economics Review 2015; 5:1-9.
- J. Hartwig. What drives health care expenditure?-Baumol’s model of "unbalanced growth" revisited. Journal of Health Economics 2008; 27: 603–623.
- WB. The World development indicators-2012. World Bank, 2012.
- M.C.Berger, & J.Messer. Public financing of health expenditures, insurance, and health outcomes. Applied Economics 2002; 34: 2105-2113.
- A.R.Sarker, R.A.Mahumud, M.Sultana, S. Ahmed, W.Ahmed & J. A.M. Khan. The impact of age and sex on healthcare expenditure of households in Bangladesh. Springer Plus 2014; 3: 1-5.
- P.Saksena, & A.Holly. The Determinants of Health Expenditure : A Country-Level Panel Data Analysis. Geneva, Switzerland, 2011.
- E.Baldacci, M.Guin-Siu, & L. De Mello. More on the effectiveness of public spending on health care and education: A covariance structure model. Journal of International Development, 2003; 15: 709–725.



