American Journal of Food Science and Health, Vol. 2, No. 6, December 2016 Publish Date: Jan. 9, 2017 Pages: 176-185
Effect of Heat-Killed Lactobacillus johnsonii No. 1088 on Gastroesophageal Reflux Disease-Related Symptoms: A Pilot Clinical Study
Yasuhiko Komatsu*, Tomoya Sasaki, Masami Ohishi
Snowden Co., Ltd., Chiyoda-ku, Tokyo, Japan
Abstract
To evaluate the efficacy of orally administered heat-killed Lactobacillus johnsonii No. 1088 (HK-LJ88) on gastroesophageal reflux disease (GERD)-related symptoms and its safety aspects, we conducted a single-blind clinical study comprising 2 dose groups (about 109 and 1010 cells/day). Thirty healthy volunteers including subjects feeling slight stomach uneasiness (22 males and 8 females), aged 24-67, not receiving medical treatment for gastric diseases and not taking drugs for gastrointestinal care, were randomly allocated 1:1 to low- or high-dose group, and instructed to ingest HK-LJ88 for 6 weeks. GERD-related symptoms were evaluated by use of the "frequency scale for the symptoms of GERD" (FSSG) and found to be significantly improved after 6 weeks in both groups. Although no significant decrease in serum gastrin concentration was observed in either group as a whole, the gastrin concentration of 7 subjects who had answered that his/her stomach condition had been improved without worsening, significantly decreased after 6 weeks. Regarding safety aspects, blood biochemical, blood cellular, and urinary tests did not show any worsening signs. Fourteen subjects experienced mild and temporal unwellness, but recovered soon. One subject in the low-dose group felt discomfort in the stomach and esophagus and voluntarily discontinued the study. This subject, however, declared afterward the tendency to feel uneasy after ingesting fermented dairy foods, which uneasiness might have reflected food allergy to lactic acid bacteria. Taken together these results suggest that ingestion of HK-LJ88 was effective to improve GERD-related symptoms of healthy volunteers, and was well tolerated up to 1010 cells/day.
Keywords
Lactic Acid Bacteria, Gastroesophageal Reflux Disease (GERD), Gastrin, Frequency Scale for the Symptoms of GERD (FSSG), Lactobacillus johnsonii No. 1088
Received: December 9, 2016
Accepted: December 20, 2016
Published online: January 9, 2017
@ 2016 The Authors. Published by American Institute of Science. This Open Access article is under the CC BY license. http://creativecommons.org/licenses/by/4.0/
Contents
1. Introduction 2. Materials and Methods 2.1. Study Design and Subjects 2.2. Materials 2.3. Measurements 2.4. Statistical Analysis 3. Results 3.1. Baseline Characteristics of the Subjects 3.2. Effect of HK-LJ88 on GERD-Related Symptoms 3.3. Effect of HK-LJ88 on Serum Gastrin Concentration 3.4. Evaluation of Safety Aspects of Oral Administration of HK-LJ88 4. Discussion 5. Conclusion Acknowledgements
1. Introduction
Gastroesophageal reflux disease (GERD) is a chronic disease caused by the flowing of gastric acid backward into the esophagus, and brings about a variety of symptoms including heartburn, taste of acid in the mouth, bad breath, chest pain, etc. Worsening of GERD results in complications including esophagitis, esophageal strictures, and Barrett's esophagus [1]. Proton pump inhibitors (PPIs) have been recommended as the first choice for therapy [1], and an another type of drug that strongly inhibits gastric acid production (potassium-competitive acid blocker; P-CAB) has recently been proposed [2, 3]. Although the efficacy of these therapeutic drugs has been widely recognized, some adverse events including hypergastrinemia are of concern in the case of their long-term usage [4-6]. So other milder ways to cope with GERD without the risk of hypergastrinemia are warranted, especially when the disease state is not so severe.
Lactobacillus johnsonii No. 1088 (LJ88) is a novel lactic acid bacterium found in the gastric juice of healthy Japanese. LJ88 has very strong resistance to acidity, inhibits growth of various virulent bacteria under mixed culture conditions in vitro, and suppresses the growth of Helicobacter pylori in the stomach of human microbiota-associated mice [7]. Moreover, oral administration of LJ88, not only as the live form but also as the heat-killed one, inhibits the PPI-induced increase in the number of gastrin-positive cells in the mouse stomach [7, 8]. Also, oral administration of heat-killed LJ88 (HK-LJ88) to germ-free mice decreases their serum concentration of gastrin, which is a hormone that stimulates the secretion of gastric acid [7, 8].
To examine the effect of HK-LJ88 on GERD-related symptoms and other health conditions in healthy Japanese volunteers including subjects feeling slight stomach uneasiness, we conducted a pilot clinical study involving oral administration of HK-LJ88 for 6 weeks. To quantitatively evaluate GERD-related symptoms, we employed a "frequency scale for the symptoms of GERD" (FSSG) scoring system, which was earlier proposed by Kusano et al. [9, 10] and has been widely used mainly in Japan as a rapid and convenient tool for the diagnosis of GERD [11]. The serum gastrin concentration was also determined to evaluate the degree of contribution of gastrin to the possible improvement of GERD-related symptoms effected by HK-LJ88. Blood biochemical, blood cellular, and urinary tests were also done to determine the safety aspects of orally administered HK-LJ88.
2. Materials and Methods
2.1. Study Design and Subjects
This was a 6-week, randomized, single-blind, parallel-group (low- and high-dose groups) study conducted between May and September 2016. This clinical study was done in compliance with the Declaration of Helsinki and the Ethical Guidelines for Medical and Health Research Involving Human Subjects (2014; Ministry of Education, Culture, Sports, Science and Technology, Japan; Ministry of Health, Labour and Welfare, Japan), and was approved by the institutional review board of Snowden Co., Ltd. Since this was a pilot clinical study conducted for the first time preliminarily to know whether HK-LJ88 was effective and safe for humans, we had not registered the study in a public database prior to the start of the study according to the exemption statement included in Part 9 of the Ethical Guidelines for Medical and Health Research Involving Human Subjects. All subjects provided written informed consent prior to participating in the study.
A total of 30 healthy Japanese peoples, who were employees of Snowden Co., Ltd., were recruited for this study. The eligibility criteria were (1) 20 - 70 years of age; (2) male or female; (3) not receiving medical treatment for gastric diseases; (4) not taking drugs for gastrointestinal care; (5) FSSG total score ≤ 20; (6) agreement to participate in the study and afford written informed consent; (7) not pregnant, not breast-feeding, or not possibly pregnant in the very near future; (8) not routinely using drugs possibly affecting the result of the study, e.g., acid reducers including H2-blockers, PPIs, P-CABs, etc.; (9) not participating in other clinical studies; and (10) not inappropriate as subjects by the decision of the study director. Regarding the eligibility criterion "5," Kusano et al. originally proposed that an FSSG total score of ≥ 8 might be used as a cut-off value for probable GERD. But in this present study, since all subjects should have had no mediations or medical treatment with respect to the stomach, we considered them as healthy subjects but feeling slight stomach uneasiness.
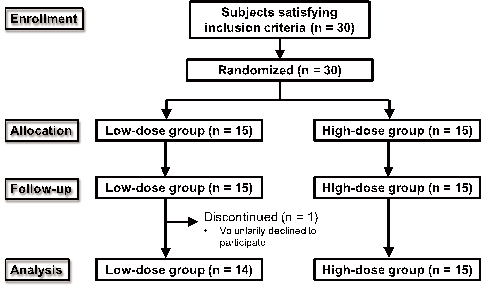
Figure 1. Flow diagram of the study.
The randomization was performed in secret to any subject based on random numbers generated by a computer, and the subjects were allocated 1:1 to a low- or high-dose group. After randomization, both groups started to ingest test samples containing about 109 and 1010 cells of HK-LJ88, respectively. One out of 15 subjects in the low-dose group voluntarily discontinued the study because of feeling discomfort in the stomach and esophagus. Finally, 29 subjects (14 and 15 for low- and high-dose groups, respectively) completed the study and were used for data analysis (Figure 1).
2.2. Materials
We used sachets each containing about 5 × 108 and 5 × 109 cells of HK-LJ88 to attain 109 and 1010 cells/day for low- and high-dose groups, respectively, by ingestion of 2 sachets/day. LJ88 was cultured in a stirred tank fermenter, washed with water, autoclaved, lyophilized with excipients, and finally triturated and diluted to afford HK-LJ88 raw material powder guaranteeing a cell number > 1010 cells/g (determined to be 1.36 × 1010/g). The low-dose sachet contained 50 mg of HL-LJ88 raw material powder, 450 mg of diluent (potato starch: reduced malt sugar syrup = 8:2), 338 mg of lactose, 350 mg of β-cyclodextrin, and 12 mg of silicon dioxide powder; and the high-dose one, 500 mg of HL-LJ88 raw material powder, 338 mg of lactose, 350 mg of β-cyclodextrin, and 12 mg of silicon dioxide powder.
2.3. Measurements
To quantitatively evaluate GERD-related symptoms, we employed the FSSG scoring system proposed by Kusano et al. [9, 10]. This system consists of 12 questions on a 5-point scale (never, occasionally, sometimes, often, and always), and scores of 0 to 4 were assigned to each of them. Since 7 [Do you get heartburn?; Do you sometimes subconsciously rub your chest with your hand?; Do you get heartburn after meals?; Do you have an unusual (e.g., burning) sensation in your throat?; Do some things get stuck when you swallow?; Do you get bitter liquid (acid) coming up into your throat?; Do you get heartburn if you bend over?] and 5 [Does your stomach get bloated?; Does your stomach ever feel heavy after meals?; Do you ever feel sick after meals?; Do you feel full while eating meals?; Do you burp a lot?] questions are related to acid reflux and acid-related dyspeptic symptoms, respectively [10], we also used these subscores in addition to total score to evaluate the effect of HK-LJ88. FSSG scoring was done before and 3 and 6 weeks after the onset of HK-LJ88 administration.
In addition to the FSSG scoring system, 3 fundamental questions concerning the stomach condition were asked before the onset of HL-LJ88 ingestion and 1 day, 3 weeks, and 6 weeks after it: "stomach condition (good, normal, not bad, bad)"; "heartburn (not suffered, occasionally, frequently, at all times)"; and "change in stomach condition after ingestion of HK-LJ88 [Yes (improved, worsened), No]", which was not asked before HK-LJ88 ingestion.
Since previously reported animal experiments suggested that oral administration of HK-LJ88 decreases the serum gastrin concentration in germ-free mice [7], we determined the fasting serum gastrin concentration before and 6 weeks after the onset of HK-LJ88 ingestion to know the extent of the contribution of gastrin to the possible improvement of the subjects’ stomach condition.
To examine the safety aspects of HK-LJ88 ingestion, we also performed blood biochemical, blood cellular, and urinary tests before and 6 weeks after the onset of HK-LJ88 ingestion under the fasting condition. As blood biochemical tests, total protein, albumin, total bilirubin, aspartate aminotransferase (AST), alanine aminotransferase (ALT), γ-glutamyltransferase (γ-GTP), amylase, total cholesterol, high-density lipoprotein (HDL) cholesterol, low-density lipoprotein (LDL) cholesterol, triglyceride, urea nitrogen, creatinine, uric acid, sodium (Na), chloride (Cl), potassium (K), glucose, and C-reactive protein (CRP) levels were determined. As blood cellular tests, white blood cell count, red blood cell count, hemoglobin content, hematocrit, mean corpuscular volume (MCV), mean corpuscular hemoglobin (MCH), mean corpuscular hemoglobin concentration (MCHC), platelet count, and leukocyte counts (neutrophil, eosinophil, basophil, monocyte, and lymphocyte) were determined. For the urinary tests, urobilinogen, urine protein, pH, uric blood, ketone body, bilirubin, and glucose were determined. Furthermore, subjects were advised to keep a diary about their health condition every day throughout the study period.
2.4. Statistical Analysis
Significance of difference between groups was determined by performing the Mann Whitney U test. Significance of a change from baseline values was determined by use of the Wilcoxon signed-rank test with the Bonferroni correction. Chi-squared test was used for analyzing the rate of occurrence data. Statistical analyses were performed by using R statistical software [12] (Mann Whitney U test and Wilcoxon signed-rank test) or Microsoft Excel (Chi-squared test).
3. Results
3.1. Baseline Characteristics of the Subjects
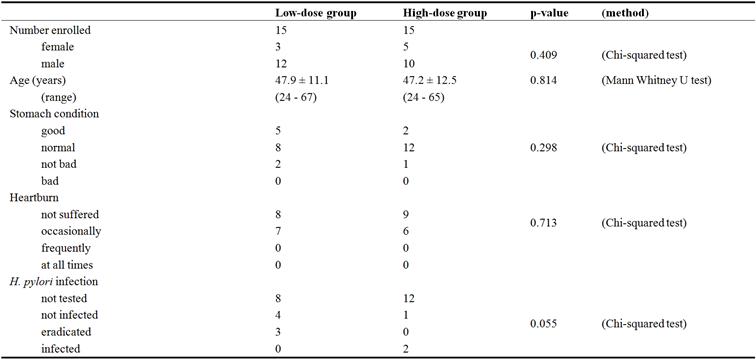
Table 1 summarizes the baseline characteristics of the subjects who participated in this study. Each group consisted of 15 subjects, where the ratios of sex and age were not significantly different from each other (p = 0.409 and 0.814, respectively). Answers to the questions about the stomach (i.e., stomach condition, heartburn, and H. pylori infection) were also not significantly different from each other (p = 0.298, 0.713, and 0.055, respectively). Regarding H. pylori infection, totally 67% of the subjects answered as "not tested", and so we did not take the states of infection by H. pylori into account for the bases of data analyses in this study.
Table 1. Baseline characteristics at screening.
3.2. Effect of HK-LJ88 on GERD-Related Symptoms
Table 2 summarizes the answers to the 3 fundamental questions before and 1 day, 3 weeks, and 6 weeks after the onset of HK-LJ88 ingestion. No significant changes were observed in the answers to the question about the "stomach condition" itself. However, the answers to the question about "heartburn" significantly changed in the low-dose group (p = 0.00017), i.e., a decrease in "occasionally" (from 7 to 2) and an increase in "not suffered" (from 7 to 12). In the high-dose group, though no significant changes were observed, the number answered "occasionally" decreased from 6 to 3 compensating "not suffered". Regarding the answers to the question about "change in stomach condition after ingestion", 5 and 3 subjects of low- and high-dose groups, respectively, answered "improved" after 6 weeks. Since 1 of them (high-dose group) answered "worsened" after 3 weeks, totally 7 subjects (5 and 2 of low- and high-dose groups, respectively) answered that his/her stomach condition had been improved without worsening.
Table 2. Questionnaire.
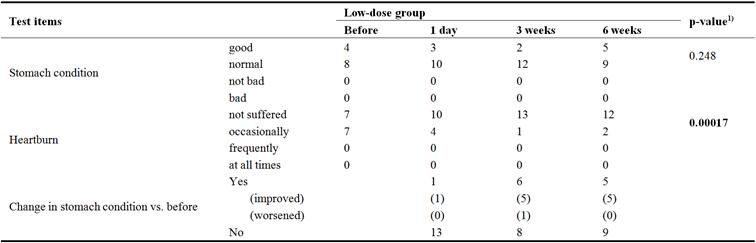
Table 2. Continued.
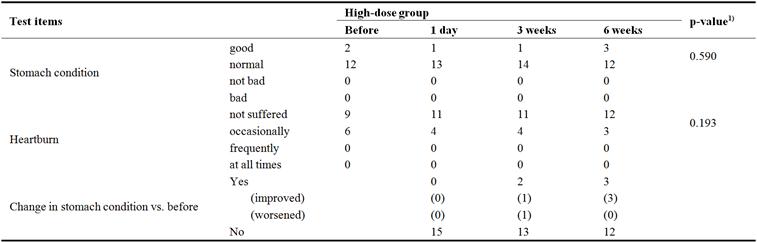
1) Chi-squared test (p-values < 0.05 are in bold type).
Figure 2 shows the changes in the FSSG total score (Figure 2A), FSSG subscores concerning acid reflux (Figure 2B), and acid-related dyspeptic symptoms (Figure 2C). As shown in these figures, in both groups the FSSG total score and the subscore concerning dyspeptic symptoms significantly decreased after 6 weeks (indicated as 6W) compared with the scores before ingestion (indicated as 0W). Table 3 summarizes the results with all p-values among the time points, indicating that no significant differences were observed between groups at other time points. Moreover, no significant differences in changes in scores were observed between groups.
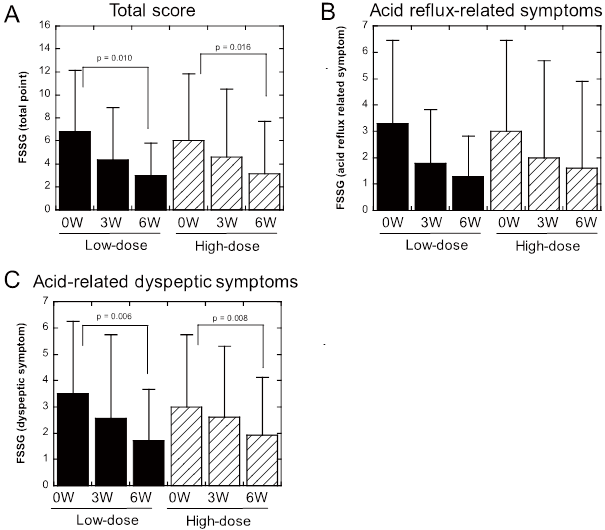
Figure 2. Effects of oral administration of heat-killed LJ88 on FSSG scores. (A) FSSG total scores, (B) FSSG subscores concerning acid reflux-related symptoms, and (C) FSSG subscores concerning acid-related dyspeptic symptoms. Each bar represents mean with S.D.
Table 3. Frequency scale for the symptoms of GERD (FSSG).
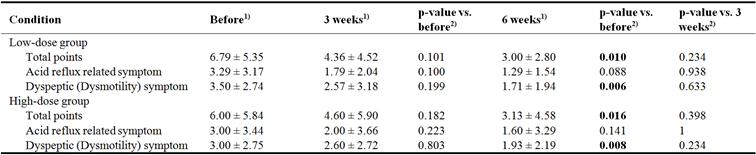
1) mean ± S.D.
2) Wilcoxon signed-rank test with Bonferroni correction (p-values < 0.05 are in bold type).
3.3. Effect of HK-LJ88 on Serum Gastrin Concentration
Figure 3 shows the serum gastrin concentrations before (indicated as 0W) and 6 weeks (indicated as 6W) after the onset of HK-LJ88 ingestion. When data from all subjects who completed the study (n = 14 and 15 for low- and high-dose groups, respectively) were analyzed, no significant changes in serum gastrin concentrations were observed in either group (Figure 3A). However, in the 7 subjects who answered that his/her stomach condition had been improved without worsening (see the 1st paragraph of the previous section and Table 1), their serum gastrin concentration significantly decreased after 6 weeks compared with that before ingestion (Figure 3B; p = 0.0469). No significant differences in changes in serum gastrin concentration were observed between groups as were FSSG scores.
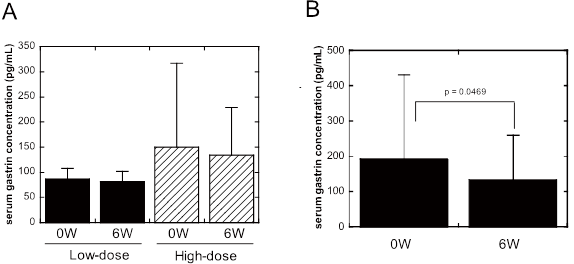
Figure 3. Effects of oral administration of heat-killed LJ88 on serum gastrin concentration. (A) Data obtained from all subjects completed the study (n = 14 and 15 for low- and high-dose groups, respectively). (B) Data obtained from 7 subjects (5 and 2 from low- and high-dose groups, respectively) who answered that his/her stomach condition had been improved without worsening. Each bar represents mean with S.D.
3.4. Evaluation of Safety Aspects of Oral Administration of HK-LJ88
Tables 4, 5, and 6 summarize the results of blood biochemical, blood cellular, and urinary tests, respectively, determined before and 6 weeks after the onset of HK-LJ88 ingestion. Among them, blood triglyceride, potassium, glucose, MCHC, platelets, and monocytes (%) were significantly changed after 6 weeks compared with their values before ingestion in the low-dose group. In the high-dose group, only blood glucose was significantly decreased after 6 weeks compared with the value before ingestion. Although these changes were statistically significant, the extents of changes other than in triglycerides was very small (0.60-11%) and within normal ranges. On the other hand, the blood triglyceride level of the low-dose group before ingestion of HK-LJ88 was higher than that of high-dose group (204 ± 163 vs. 84 ± 40; p = 0.00133), and the change was not small (about 28%). Moreover, the extents of changes in triglyceride levels were significantly different between groups (-58.6 ± 119.8 vs. 8.3 ± 29.1; p = 0.0359). However, since such a decrease in triglyceride level is not a sign of worsening of health condition, this could not be thought as an adverse effect of HK-LJ88. Fourteen subjects experienced mild and temporal unwellness (e.g., stomachache, heartburn, loose stool, constipation, headache, and/or common cold), but all recovered soon (within several days) and completed the study without further problems. One subject in the low-dose group, who declared afterward the tendency to feel uneasiness by ingestion of fermented dairy foods, felt discomfort in the stomach and esophagus and voluntarily discontinued the study. This might be the exceptional case of a kind of suspicious food allergy to lactic acid bacteria, because ingestion of a test sample prepared without HK-LJ88 did not cause such a discomfort, but a health food containing other lactic acid bacteria did.
Table 4. Blood biochemical test.
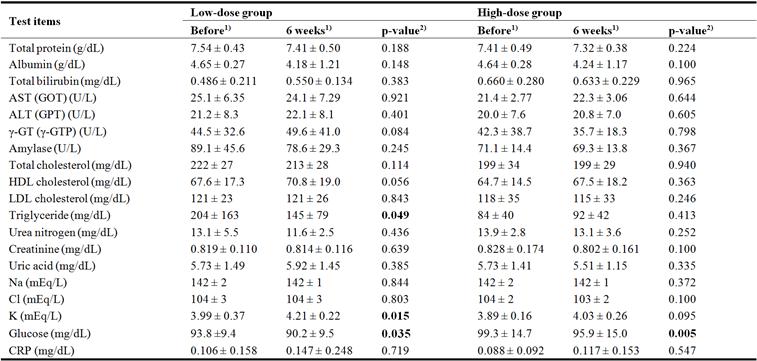
1) mean ± S.D.
2) Wilcoxon signed-rank test (p-values < 0.05 are in bold type).
Table 5. Blood Cellular test.
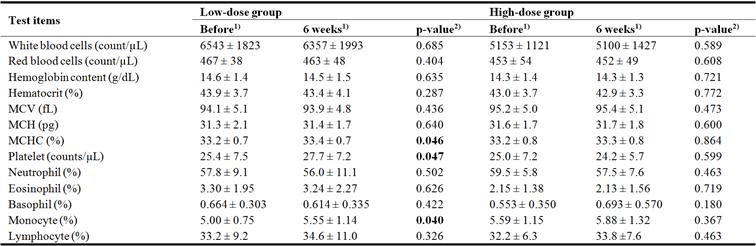
1) mean ± S.D.
2) Wilcoxon signed-rank test (p-values < 0.05 are in bold type).
Table 6. Urinary test.
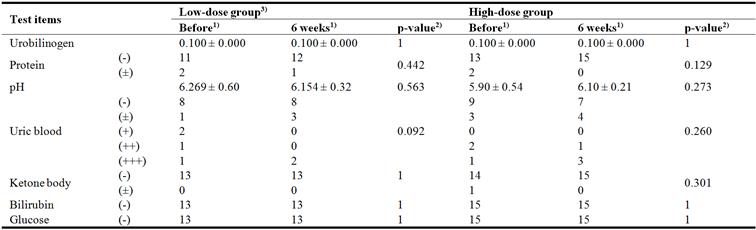
1) mean ± S.D (Urobilinogen and pH), counts (Others)
2) Wilcoxon signed-rank test (Urobilinogen and pH), Chi-squared test (Others)
3) Data from one female subject of low-dose group are omitted from the table, as she could not take the urinary test at 6 weeks because of menstruation.
4. Discussion
This was the first pilot clinical study to evaluate the efficacy toward GERD-related stomach symptoms and safety of daily ingestion of HK-LJ88. When HK-LJ88 was orally administered for 6 weeks to healthy Japanese volunteers including subjects feeling slight stomach uneasiness, FSSG scores (both total score and acid-related dyspeptic one) were significantly improved in both low- and high-dose groups (administered about 109 and 1010 cells/day, respectively). The stratified analysis of serum gastrin concentration in 7 subjects whose stomach conditions had been improved without worsening showed that their serum gastrin concentration significantly decreased after ingestion of HK-LJ88 for 6 weeks. Furthermore, no serious adverse events were observed related to ingestion of HK-LJ88, though one subjects suffered from a probable food allergy reaction to lactic acid bacteria. Therefore, HL-LJ88 can be considered to be effective to improve the stomach condition related to GERD at the doses ≥ about 109 cells/day, and well tolerated up to 1010 cells/day.
Some lactic acid bacteria and bifidobacteria have been reported to have beneficial effects on the stomach. One of the well reported effects of lactic acid bacteria on the stomach is their anti-H. pylori activity, exemplified by Lactobacillus gasseri OLL2716, Lactobacillus johnsonii La1, and our LJ88 [7, 8, 13, 18]. Among them L. gasseri OLL2716 has been reported to improve dyspeptic symptoms in H. pylori-infected patients when administered as the living form supplement in yogurt [19], and to prevent chronic gastric ulcer in rats by living forms of the bacteria but not by γ-ray radiated dead ones [20]. Bifidobacterium bifidum BF-1 (or B. bifidum YIT10347) also has been reported to improve experimental gastric injury in rats [21, 22], to suppress inflammatory cytokine (IL-8) production from stomach epithelial cell lines induced by H. pylori [23], and to alleviate gastric symptoms in human subjects taking no medication [24]. However, these studies were all performed with live bacteria, in contrast to the present study in which we observed that the dead form of a lactic acid bacterium, HK-LJ88, improved the stomach condition in humans. To our knowledge, this is the first report of such an effect of dead bacteria.
Animal studies have shown that LJ88 decreases the number of gastrin-positive cells in the stomach to bring about a reduction in the serum gastrin concentration [7]. Since gastrin is a hormone that stimulates gastric acid production from the stomach, this decrease in the serum concentration of gastrin is thought to be responsible for the reduced gastric acid production [7]. Such an effect of LJ88 is not exclusive to its living form, but also exerted by the heat-killed one [7, 8]. In the present study we measured the fasting serum gastrin concentration before and 6 weeks after the onset of HK-LJ88 ingestion, and we found no significant decrease in it in either group as a whole, whereas the FSSG sores were significantly improved by ingesting HK-LJ88 in both groups. However, the gastrin concentration of the 7 subjects who had answered that his/her stomach condition had been improved without worsening, significantly decreased after 6 weeks. These results suggest that although the gastrin-reducing effect of HK-LJ88 might contribute to improve stomach condition of healthy subjects in part, other mechanisms are also possibly responsible for the clinical effect of HK-LJ88. One possible mechanism might be its probable anti-inflammatory activity as reported to manifest in B. bifidum BF-1 [23]. Full understanding of the mechanisms by which HK-LJ88 improves the stomach condition should be elucidated in the future.
Regarding safety aspects of HK-LJ88, 14 subjects experienced mild and temporal unwellness, but recovered soon. Blood biochemical, blood cellular, and urinary tests did not show any sign of worsening of the health condition related to HK-LJ88 ingestion in either low- or high-dose group. But one subject in the low-dose group, who declared afterward the tendency to feel uneasiness by ingestion of fermented dairy foods, felt discomfort in the stomach and esophagus and voluntarily discontinued the study. Since this subject is suspected to have a kind of allergy to lactic acid bacteria, it should be kept in mind that there might exist such people who do not tolerate lactic acid bacteria including LJ88. However, taken together our data indicate that orally administered KH-LJ88 is well tolerated and safe up to 1010 cells/day.
There exist some limitations in this study. For example, we allowed the inclusion of subjects having FSSG total scores of ≤ 20, which actually ranged from 0 to 20. But since Kusano et al. proposed that FSSG total scores of ≥ 8 should be thought as probable GERD [9], subjects having baseline FSSG total scores of ≥ 8 might have been omitted to ensure strictly healthy subjects. The number of such subjects was 9 in this study. On the other hand, we also included subjects having very low FSSG total scores, who should be thought of as people not suffering from any stomach uneasiness related to GERD. For example, the number of subjects having FSSG total scores of ≤ 2 was 9 in this study. In a future clinical study, these subjects with very low FSSG total scores should be excluded as well. Regarding the serum gastrin concentration, 2 subjects in the high-dose group had extremely high gastrin concentrations (230 and 730 pg/mL, respectively). Although they had not received any medical treatment for gastric diseases, and had not taken drugs for gastrointestinal care, such subjects should have been excluded from the study. Furthermore, to know the ability of HK-LJ88 to reduce the serum gastrin level, a lower limit for its level should have been set as inclusion criteria, e.g., ≥ 80 pg/mL. Based on the above considerations, both lower and upper limits for both FSSG total score and serum gastrin concentration should be taken into consideration in the future detailed clinical studies. Moreover, randomized, double-blind, placebo-controlled studies should be done by recruiting a larger number of subjects to further confirm the effectiveness of HK-LJ88 to improve the stomach health condition.
5. Conclusion
To evaluate the efficacy of orally administered heat-killed HK-LJ88 on GERD-related symptoms and its safety aspects, we conducted a single-blind clinical study comprising 2 dose groups (about 109 and 1010 cells/day). GERD-related symptoms were evaluated by use of the FSSG and found to be significantly improved after 6 weeks in both groups. Although no significant decrease in serum gastrin concentration was observed as a whole, the gastrin concentration of 7 subjects who had answered that his/her stomach condition had been improved without worsening, significantly decreased after 6 weeks. Regarding safety aspects, blood biochemical, blood cellular, and urinary tests did not show any worsening signs. Some subjects experienced mild and temporal unwellness, but recovered soon. One subject in the low-dose group felt discomfort in the stomach and esophagus and voluntarily discontinued the study, whereas this uneasiness might have reflected food allergy to lactic acid bacteria. Taken together these results suggest that ingestion of HK-LJ88 was effective to improve GERD-related symptoms of healthy volunteers, and was well tolerated up to 1010 cells/day.
Acknowledgements
We thank Dr. Shigeki Mabuchi at Tokyo Total Life Clinic, Tokyo, Japan for performing blood biochemical, blood cellular, and urinary tests and for helpful advice regarding this study.
References
- Kahrilas P. J., Shaheen N. J., Vaezi M. F., Hiltz S. W., Black E., Modlin I. M., Johnson S. P., Allen J., Brill J. V. (2008). American Gastroenterological Association Medical Position Statement on the management of gastroesophageal reflux disease. Gastroenterology. 135 (4): 1383-1391.
- Garnock-Jones K. P. (2015). Vonoprazan: first global approval. Drugs. 75 (4): 439-443.
- Ashida K., Sakurai Y., Nishimura A., Kudou K., Hiramatsu N., Umegaki E., Iwakiri K., Chiba T. (2015). Randomised clinical trial: a dose-ranging study of vonoprazan, a novel potassium-competitive acid blocker, vs. lansoprazole for the treatment of erosive oesophagitis. Aliment Pharmacol Ther. 42 (6): 685-695.
- Ashida K., Sakurai Y., Hori T., Kudou K., Nishimura A., Hiramatsu N., Umegaki E., Iwakiri K. (2016). Randomised clinical trial: vonoprazan, a novel potassium-competitive acid blocker, vs. lansoprazole for the healing of erosive oesophagitis. Aliment Pharmacol Ther. 43 (2): 240-251.
- Fossmark R., Johnsen G., Johanessen E., Waldum H. L. (2005). Rebound acid hypersecretion after long-term inhibition of gastric acid secretion. Aliment Pharmacol Ther. 21 (2): 149-154.
- Waldum H. L., Arnestad J. S., Brenna E., Eide I., Syversen U., Sandvik A. K. (1996). Marked increase in gastric acid secretory capacity after omeprazole treatment. Gut. 39 (5): 649-653.
- Aiba Y., Nakano Y., Koga Y., Takahashi K., Komatsu Y. (2015). A highly acid-resistant novel strain of Lactobacillus johnsonii No. 1088 has antibacterial activity, including that against Helicobacter pylori, and inhibits gastrin-mediated acid production in mice. Microbiology Open. 4: 465-474.
- Komatsu Y., Aiba Y., Nakano Y., Koga Y. Probiotics, prebiotics, and biogenics for the stomach. In: Rao V, Rao LG, editors. Prebiotics and Probiotics in Human Nutrition and Health. Rijeka, Croatia: InTech; 2016. p. 363-381.
- Kusano M., Shimoyama Y., Sugimoto S., Kawamura O., Maeda M., Minashi K., Kuribayashi S., Higuchi T., Zai H., Ino K., Horikoshi T., Sugiyama T., Toki M., Ohwada T., Mori M. (2004). Development and evaluation of FSSG: frequency scale for the symptoms of GERD. J Gastroenterol. 39 (9): 888-891.
- Kusano M., Shimoyama Y., Kawamura O., Maeda M., Kuribayashi S., Nagoshi A., Zai H., Moki F., Horikoshi T., Toki M., Sugimoto S., Mori M. (2007). Proton pump inhibitors improve acid-related dyspepsia in gastroesophageal reflux disease patients. Dig Dis Sci. 52 (7): 1673-1677.
- Nonaka T., Kessoku T., Ogawa Y., Yanagisawa S., Shiba T., Sakaguchi T., Atsukawa K., Takahashi H., Sekino Y., Iida H., Endo H., Sakamoto Y., Koide T., Takahashi H., Yoneda M., Maeda S., Nakajima A., Gotoh E., Inamori M. (2013). Comparative Study of 2 Different Questionnaires in Japanese Patients: The Quality of Life and Utility Evaluation Survey Technology Questionnaire (QUEST) Versus the Frequency Scale for the Symptoms of Gastroesophageal Reflux Disease Questionnaire (FSSG). J Neurogastroenterol Motil. 19 (1): 54-60.
- R_Core_Team. (2016). R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria URL https://wwwR-projectorg/.
- Fukushima Y., Yamano T., Kusano A., Takada M., Amano M., Iino H. (2004). Effect of fermented milk containing Lactobacillus johnsonii La1 (LC1) on defecation in healthy Japanese adults ---- A double blind placebo controlled study ----. Bioscience Microflora. 23 (4): 139-147.
- Felley C. P., Corthesy-Theulaz I., Rivero J. L., Sipponen P., Kaufmann M., Bauerfeind P., Wiesel P. H., Brassart D., Pfeifer A., Blum A. L., Michetti P. (2001). Favourable effect of an acidified milk (LC-1) on Helicobacter pylori gastritis in man. Eur J Gastroenterol Hepatol. 13 (1): 25-29.
- Michetti P., Dorta G., Wiesel P. H., Brassart D., Verdu E., Herranz M., Felley C., Porta N., Rouvet M., Blum A. L., Corthesy-Theulaz I. (1999). Effect of whey-based culture supernatant of Lactobacillus acidophilus (johnsonii) La1 on Helicobacter pylori infection in humans. Digestion. 60 (3): 203-209.
- Sakamoto I., Igarashi M., Kimura K., Takagi A., Miwa T., Koga Y. (2001). Suppressive effect of Lactobacillus gasseri OLL 2716 (LG21) on Helicobacter pylori infection in humans. J Antimicrob Chemother. 47 (5): 709-710.
- Fujimura S., Kato S., Oda M., Miyahara M., Ito Y., Kimura K., Kawamura T., Ohnuma M., Tateno H., Watanabe A. (2006). Detection of Lactobacillus gasseri OLL2716 strain administered with yogurt drink in gastric mucus layer in humans. Lett Appl Microbiol. 43 (5): 578-581.
- Kato-Mori Y., Orihashi T., Kanai Y., Sato M., Sera K., Hagiwara K. (2010). Fermentation metabolites from Lactobacillus gasseri and Propionibacterium freudenreichii exert bacteriocidal effects in mice. J Med Food. 13 (6): 1460-1467.
- Takagi A., Yanagi H., Ozawa H., Uemura N., Nakajima S., Inoue K., Kawai T., Ohtsu T., Koga Y. (2016). Effects of Lactobacillus gasseri OLL2716 on Helicobacter pylori-Associated Dyspepsia: A Multicenter Randomized Double-Blind Controlled Trial. Gastroenterol Res Pract. 2016: 7490452.
- Uchida M., Shimizu K., Kurakazu K. (2010). Yogurt containing Lactobacillus gasseri OLL 2716 (LG21 yogurt) accelerated the healing of acetic acid-induced gastric ulcer in rats. Biosci Biotechnol Biochem. 74 (9): 1891-1894.
- Nagaoka M., Hashimoto S., Watanabe T., Yokokura T., Mori Y. (1994). Anti-ulcer effects of lactic acid bacteria and their cell wall polysaccharides. Biol Pharm Bull. 17 (8): 1012-1017.
- Gomi A., Harima-Mizusawa N., Shibahara-Sone H., Kano M., Miyazaki K., Ishikawa F. (2013). Effect of Bifidobacterium bifidum BF-1 on gastric protection and mucin production in an acute gastric injury rat model. J Dairy Sci. 96 (2): 832-837.
- Shirasawa Y., Shibahara-Sone H., Iino T., Ishikawa F. (2010). Bifidobacterium bifidum BF-1 suppresses Helicobacter pylori-induced genes in human epithelial cells. J Dairy Sci. 93 (10): 4526-4534.
- Gomi A., Iino T., Nonaka C., Miyazaki K., Ishikawa F. (2015). Health benefits of fermented milk containing Bifidobacterium bifidum YIT 10347 on gastric symptoms in adults. J Dairy Sci. 98 (4): 2277-2283.



