American Journal of Food Science and Health, Vol. 2, No. 5, October 2016 Publish Date: Aug. 19, 2016 Pages: 117-122
The Effects of Health Care Costs on Health Status in Selected Developed Countries
Arash Ketabforoush Badri1, *, Aidin Poorabdollahi Sheshgelani2
1Department of Economics, College of Management and Accounting, Qazvin Branch, Islamic Azad University, Qazvin, Iran
2Master of Executive Management, Department of Management, Tabriz branch, Islamic Azad University, Tabriz, Iran
Abstract
Health can be considered an important component of human capital and normally it is expected that healthy people who are working with a certain amount of production factors, are more productive than patients labor. Healthy people are usually more motivated to earn money, harder working and more efficient. In addition, increasing investment in health care can enhance the efficiency of other investments in training health human resources in areas such as public and specialized education. Accordingly, this paper is trying to examine the effects of health care costs on health status in selected developed countries in 2000 to 2014 using panel data and GMM methods. The results show that public health expenditures, private health expenditures, GDP per capita and education and human development have negative effects on mortality rate and the population over 65 years has a positive effect on mortality rate. The results of GMM methods show that mortality rate with a time lag and the population over 65 years have postive effects and public health expenditures, private health expenditures, GDP per capita and education and human development have negative effects on mortality rate in studied countries.
Keywords
Health Care Costs, Health Status, Panel Data, GMM
Received:July 30, 2016
Accepted: August 7, 2016
Published online: August 19, 2016
@ 2016 The Authors. Published by American Institute of Science. This Open Access article is under the CC BY license. http://creativecommons.org/licenses/by/4.0/
Contents
1. Introduction
Health status of any person directly or indirectly linked to a set of variables that are related to health. These factors include behavioral, environmental and economic factors. Among these factors can be cited health expenditure. Improving the health status is not the only determinant the government the level of health expenditure; but also political and economic factors contribute to meeting the government's decision to enforce health policy (Rivera and Currais, 2004, 874).
Health of each individual which in turn depends on a set of behavioral and environmental variables, be a part of a person's human capital and naturally in the process of economic growth to improve the efficiency of enterprises. Based on this fact, some theorists have considered the health factor, as one of the components of human capital in economic growth models (Khalili and Souri, 2006, 4).
The most important achievement of improved health are reducing the days missed from work due to illness (sick leave), increased productivity, better able to seize opportunities to work with higher incomes and increasing the lifespan of workers and employees (Raeesipour and Pazhouyan, 2013, 45).
Health costs, increases the health of labor force, and through this, the more healthy people with higher physical and mental ability entered the production process and this issue can have a positive impact on increasing productivity and economic growth. More healthy persons provide more appropriate mixed, factors of production, increase productivity and economic growth (Sarlak and Kiyani, 2015, 172).
Finlay (2007) believes that, enjoy good health and long, is one of the principles of human experience. Healthy people have more energy and freshness and have a positive outlook towards life better.
Health of society people leads to a reduction in costs of illness and from location of these savings can be made newer investments in various sectors and by increasing the production capacity has accelerated future growth.
For this purpose, this study tries to examine the fffects of health care costs on health status in 10 selected developed countries in period 2000-2014 using panel data and GMM methods.
2. Literature Review
Health an issue that is closely related to the progress and development, including growth and economic development. Healthy people are more energetic and enthused and motivated to work and operate. Also, the direct and indirect costs to the national income and leads to the growth and development decreased. That is why, today all societies have paid special attention to enhancing the health indices. In economic literature is presented to health, various definitions. The World Health Organization defines health as not just the absence of illness, but the welfare of complete physical, mental and social (WHO, 2010).
Health as a commodity to apply both for consumption and investment. From a consumer perspective, people are looking for a healthy because in this case to improve their quality of life and pleasure are more favorable. From the perspective of investment, the relationship between time and health, so that, if a person's health is good, time will be less disease and more days to work and earn more money and have a rest and recreation (Lotfalipour and et al, 2011, 59).
Chadwick in 1842 with the publication of an article, introduced health expenditure as an investment in human capital (Spence and Lewise, 2009). In spite of this introduction of health and growth in theory, only in recent decades has been conducted, a series of scattered studies on the health effects on economic growth.
Health status of a person, depends on, to a set of behavioral variables, environmental and economic (including health expenditures) affecting him. Capital health of any person as part of his human capital contribute to economic growth. Due to this, it could be a result of human capital and health capital in the economic development functions.
Schultz believes that human capital does not occur only through the accumulation of knowledge and education. In his view, education and health is one of the investment in human capital. Belag also believes that other forms of investment in human capital to foster personal property and help improve the quality of the labor force. The health workforce and health care, job training and job experience can increase their income. Therefore, they should also be considered as investment in human capital (Emadzadeh et al., 2011, 924).
Attention the use of health and welfare in the field of economy began when as Rosenthal in 1960, in an article health and society, studied the history of health in the economy of United States (Ghanbari and Basakha, 2006, 190).
Arrow (1963), with release paper of the government's involvement in health care justified and posed the question which theoretically would provide the health service should be done by the government or the free market? In this decade, economists over how to allocate the performance and health costs and paid to the effects of improving health on economic growth. Also, Solow (1965) for the first time, enter the human capital in the production function, and measured the contribution of education to economic growth in this way.
Grossman (1972) was the first person who entered, health capital in the production of utility functions. He believed that the situation of human health is considered as a reserve and Therefore, health, is capital goods which produces a healthy time. Therefore, it can be entered in the production and utility function. He also believes that capital of knowledge and education is affected market and non-market labor productivity. However, capital of individual health plays an important role in determining when a person is able to monetize it. Grossman considers gross investment in health and health which leads to the production of goods is a function of medical care, proper diet, exercise, healthy recreational activities and so on. In his view health will be asked by different people the two main causes. First, health itself directly into a commodity and utility functions, so that the disease will lead to a decrease in the utility. The second reason is that health is an investment product that determines the ability to perform non-economic and economic activities in the community. In other words, capital of individual health reduces the time lost (due to illness) for him and the proceeds from this time can be regarded as an indicator for increasing individual productivity. That can proceeds from this time to take into account as an indicator of improved individual performance.
Kofi and Ramu (2016) studied the effect of public health expenditure on health status in Ghana using OLS method in period 1990-2012. The regression estimates suggest that real per capita income, public health expenditure, education and female presence in the labour market were negatively related to infant mortality rate. However, the elasticity coefficients of female participation in the labour market and real per capita income were statistically insignificant at 5% level.
Nahidi et al (2016) investigated the impact of health spending on economic growth in the period 2005-2013 using panel data for 32 selected OECD countries. The results show that health spending has a significant and positive effect on economic growth, so that an increase of 1 percent of its value, economic growth 0/04 percent increased. Also, physical capital and the working population have a significant positive effect on economic growth. However, inflation had a negative effect on economic growth, as inflation increased the rate of economic growth decreased.
Ketabforoush and Ketabforoush (2016) studied relationship between health spending and economic growth in in 24 selected countries of OECD in the period 2006-2013 using GMM methods. The results show that health spending has a significant and positive effect on economic growth, so that an increase of 1 percent of its value, economic growth 0/04 percent increased. Also, physical capital and the working population have a significant positive effect on economic growth. However, inflation has a negative effect on economic growth, as inflation increased the rate of economic growth decreased.
Makuta and O’Hare (2015) in study examine the quality of governance, public spending on health and health status in Sub Saharan Africa Using two staged least squares regression technique on panel data from 43 countries in SSA over the period 1996–2011. The results show that Public spending on health has a statistically significant impact in improving health outcomes. Its direct elasticity with respect to under-five mortality is between −0.09 and −0.11 while its semi-elasticity with respect to life expectancy is between 0.35 and 0.60.
Barouni et al (2015) studied the effects of public and private health expenditure on human development index for 52 selected countries of the world in three income groups high, medium and low in period 2000 to 2010 using panel data method. Results indicate that public and private health expenditures have postive effects of on human development index in studied countries.
Homaie Rad et al (2013) in a study comparison of the effects of public and private health expenditures on the health status using panel data analysis in eastern mediterranean countries between 1995 to 2010. The study findings showed that the public health expenditures in the EMR countries improved health outcome, while the private health expenditures did not have any significant relationship with health status, so often increasing the public health expenditures leads to reduce IMR. But this relationship was not significant because of contradictory effects for poor and wealthy peoples.
Cevik and Tasar (2013) aim to analyze the effect of government spending on health-care on health outcomes with cross-national comparison. They found government health spending as a share of GDP is negatively associated with lower level of under-5 mortality by elasticities of from -0.17 to -0.22. The elasticity is -0.20 for infant mortality. When government spending as a share total health expenditures is used as estimator, elasticities are -0.33 for under-5 mortality and -0.23 and -.0.32 for infant mortality.
Novignon et al (2012) studied the effects of public and private health care expenditure on health status in sub-Saharan Africa. The empirical evidence presented above suggests that the exact relationship between health care spending and health outcomes is not clear, especially at the macro level.
3. Material and Methods
3.1. Data and Statistics
The population of this study are 10 selected countries of the OECD, including Japan, Austria, Spain, Finland, France, Italy, Iceland, Norway, Netherlands, Portugal. The period has been used 2000-2014. This is the time series data collected from WDI2016 and OECD site statistics. The model presented in this study, inspired by Novignon et al (2012), Homaie Rad et al (2013) and Mohammadzadeh et al (2014) as follows:
L![]() =
=![]() +
+ ![]() +
+ ![]()
L![]() = logarithm of infant mortality rate of the countries
= logarithm of infant mortality rate of the countries
L![]() = logarithm of public health expenditures per capita of country i
= logarithm of public health expenditures per capita of country i
L![]() = logarithm of private health expenditures per capita of country i
= logarithm of private health expenditures per capita of country i
L![]() = logarithm of the proportion of people over 65 years to total population of country i
= logarithm of the proportion of people over 65 years to total population of country i
L![]() = logarithm of the gross domestic product per capita of country i
= logarithm of the gross domestic product per capita of country i
L![]() = logarithm of human capital by multiplying the enrollment rates in education in adult literacy rates of country i
= logarithm of human capital by multiplying the enrollment rates in education in adult literacy rates of country i
![]() = random error
= random error
3.2. Estimation Method
Panel data is data from a (usually small) number of observations over time on a (usually large) number of crosssectional units like individuals, households, firms, or governments. In other words panel data analysis is a method of studying a particular subject within multiple sites, periodically observed over a defined time frame. With repeated observations of enough cross-sections, panel analysis permits the researcher to study the dynamics of change with short time series. The combination of time series with cross-sections can enhance the quality and quantity of data in ways that would be impossible using only one of these two dimensions (Gujarati, 2004).
Generalized Method of Moments (GMM) Generalized Method of Moments (GMM) refers to a class of estimators which are constructed from exploiting the sample moment counterparts of population moment conditions (some-times known as orthogonally conditions) of the data generating model. GMM estimators have become widely used, for the following reasons (Hansen, 2007). First, GMM estimators have large sample properties that are easy to characterize in ways that facilitate comparison. A family of such estimators can be studied a priori in ways that make asymptotic efficiency comparisons easy. The method also provides a natural way to construct tests which take account of both sampling and estimation error. Second, in practice, researchers find it useful that GMM estimators can be constructed without specifying the full data generating process (which would be required to write down the maximum likelihood estimator). This characteristic has been exploited in analyzing partially specified economic models, in studying potentially dis specified dynamic models designed to match target moments, and in constructing stochastic discount factor models that link asset pricing to sources of macroeconomic risk. To ensure the appropriate the method for estimating the model, Wald test and Sargan test is proposed. Wald test used for the significance repressors and Sargan test is used to prove the validity of instrumental variables.
4. Results and Discussion
4.1. Checking Stationary of Variables
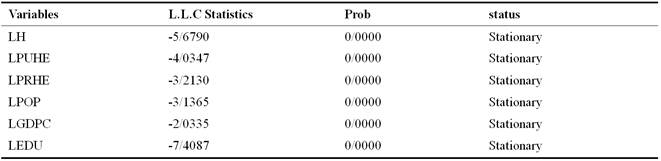
If the time series are non-stationary, the estimated coefficients will lead to a spurious regression. So before estimating the model it is required to check the stationary of all variables used in the estimates. For this purpose, the Levin, Lin & Chu (LLC), Im, Pesaran and Shin (IPS), Augmented Dickey – Fuller (ADF-Fisher), Fisher - Phillips and Peron (PP-Fisher) test presented by Maddala & Wu (1999) and Choi (2001) tests are used. These four tests are most important Common unit Root tests in panel data. Although Different methods of common unit root tests may provide conflicting results on panel data. In all these tests the null hypothesis is the presence of a unit root. This study Check the Stationary of variables by the Levin, Lin & Chu test.
Table 1. Results of stationary of variables using L.L.C test.
Sources: research findings
As stationary test results show, all variables used in the model at the level are stationary.
4.2. The Results of Panel Data
Accordingly, the results of model estimation is introduced to determine the effects of health care costs on health status using a fixed effects panel data are presented in Table 2.
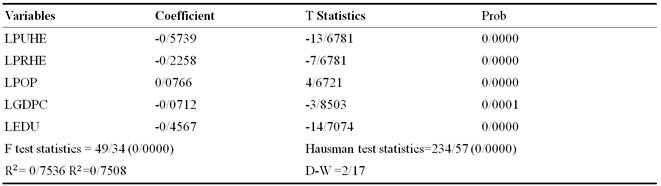
Table 2. Results of estimating effects of health care costs on health status.
Sources: research findings
According to the results of Table 2 of the F and Hausman tests, it can be said, the value of F test statistic using fixed effects would be more appropriate. Houseman also test statistic indicates the suitability of the method for estimating the fixed effects model. So, fixed effects is used in the estimation model.
All coefficients of explanatory variables are significant. The estimated coefficient for public health expenditures is -0/5. This shows that a 1% increase in public health expenditures, mortality rate 0/5% reduced. Also, 1% increase in private health expenditures, mortality rate 0/2% reduced. Based on results, public health expenditure were more than private health expenditures, reduce the mortality rate. Public health expenditure through the provision of infrastructure and public health facilities and immunization measures against various diseases can reduce the mortality rate in the countries surveyed. Also, private health expenditures can be achieved through increasing access to health services and higher quality equipment and raising awareness of their health and also have an additional impact on reducing mortality in the studied countries. The GDP per capita is negatively correlated with mortality. Because by the 1% increase in GDP per capita, the mortality rate 0/07% reduced. Also, with the increase in the population over 65 years, the mortality rate is also increasing. It should be noted, with increasing levels of education and human development, mortality rates reduced. So that a 1% increase in the level of education, mortality rate 0/4% reduced. This implies that the high level of people's knowledge and awareness of how to use sanitary facilities can reduce mortality rate in communities.
4.3. The Results of GMM Methods
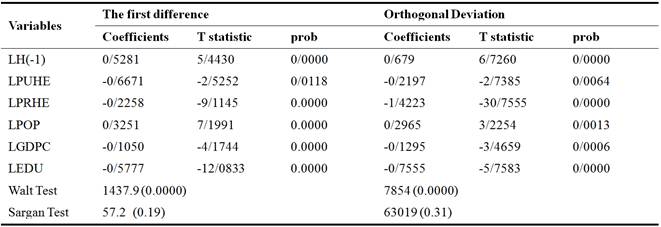
Table 3 shows the results of the effect effects of health care costs on health status with GMM method. In this table, statistics relating to the Walt and the Sargan test is given.
Table 3. Results of estimating effects of health care costs on health status using GMM.
Sources: research findings
According to the results by the first difference, coefficients of mortality rate with a time lag, public health expenditures, private health expenditures, working population, GDP per capita, education index, respectively, are 0/5, -0/6, -0/2, 0/3, -0/1 and -0/5. According to the results by the orthogonal deviation, coefficients of mortality rate with a time lag, public health expenditures, private health expenditures, working population, GDP per capita, education index, respectively, are 0/6, -0/2, -1/4, 0/2, -0/1 and -0/7. Also, the Wald test is used to determine the significance of the model that according to the P-Value in this test, the model proved to be significant. Sargan test statistic distribution χ2 is the degrees of freedom equal to the number of over-identifying restrictions and the test of the null hypothesis that there is no correlation tools disturbing components. By examining P-Value of the test; The results indicate the validity of the assumptions of estimates, namely, the tools are valid, the results confirm the validity of the results for interpretation.
5. Conclusion
Health is One of the items that can have a significant impact on economic growth, by increasing the power of national human resources. It can be said health promotion brings people are healthier and more productive. High levels of public health, may increase the individual's ability to learn, which in turn leads to significant influence in increasing the productivity of investment in education. Given the role of health in human life and the goal of economic and social development which ultimately leads to growth and social welfare, can be seen the main lines of growth and economic development mutual relationship of human capital. Health an issue that is closely related to the development, including growth and economic development. Healthy people are more energetic and enthused and motivated to work and operate. Therefore, health is the basis for job productivity, and the ability to learn in school physical, mental and essential intelligence and productivity in adulthood. This paper examined the effects of health care costs on health status in selected developed countries by using the panel data and GMM methods for the period 2000-2014. The results of the panel data showed that public health expenditures, private health expenditures, GDP per capita and education and human development have negative effects on mortality rate and the population over 65 years has a positive effect on mortality rate. The results of GMM methods showed mortality rate with a time lag and the population over 65 years have postive effect and public health expenditures, private health expenditures, GDP per capita and education and human development have negative effects on mortality rate in studied countries.
References
- Barouni, M., Harati Khalilabad, T., Harati, J. (2015), the effects of public and private health expenditure on human development index for selected countries of the world in three income groups high, medium and low, Health Management, 6, 2, 81-91.
- Bloom, D. E., Canning, D., & Sevilla, S. (2003). The effect of health on economic growth: A production function approach. World Development, 32(1), 1–13.
- Cevik, S., Tasar, O. (2013), Public Spending on Health Care and Health Outcomes: A Cross-Country Comparison, Journal of Business, Economics & Finance (2013), Vol.2 (4), 83-102.
- Emadzadeh, M., Sameti, M., Safi, D. (2011), The relationship between health spending and economic growth in Iran, Health Information Management, Vol. 8, No. 7, 928-918.
- Ghanbari, A., Basakha, M. (2006), Changes in the cost of government health effects on economic growth (1338-83 years), Journal of Economic Research Tehran University, No. 83, Summer, 187-224.
- Gujarati, D. (2003). Basic Econometrics, the McGraw-Hill.
- Homaie Rad, E., Vahedi, S., Tiemourizad, A., Esmaelzadeh, F., Hadian, M., Torabi Pour, A.(2013), Comparison of the effects of public and Private Health Expenditures on The Health Status:A Panel Data Analysis in Eastern Mediterranean Countries, International Journal of Health Policy and Management, 1(2), 163-167.
- Khalili, M., Souri, A. (2006), To estimate the efficiency and effectiveness of Iran's economy and its relationship with government spending. Economic Research, Volume 3, Issue 74, 1-23.
- Ketabforoush Badri, A., Ketabforoush Badri, S. (2016), Health Spending and Economic Growth in Selected OECD Countries, American Journal of Clinical Neurology and Neurosurgery, Vol.2, No.1, 5-9.
- Kofi Boachie, M., Ramu, K.(2016), Effect of Public helath expendture on health status in Ghana, International Journal of Health, $(1), 6-11.
- Lotfalipour, M., Fallahi, M., Borji, M. (2011), The effect of health indicators on economic growth, health management, 14 (46), 57-70.
- Makuta, I., O’Hare, B. (2015), Quality of governance, public spending on health and health status in Sub Saharan Africa: a panel data regression analysis, BMC Public Health, 15, 932, 1-11.
- Nahidi, M., Ketabforoush Badri, A., Ketabforoush Badri, S. (2016), investigated the impact of health spending on economic growth of OECD countries, Journal of Global Economics, Management and Business Research, Vol.5, Issue 4, 280-283.
- Novignon, J., Olakojo, S., Nonvignon, J. (2012), The Effects of Public and Private Health Care Expenditure and Health Status in Sub-Sahara Africa: New Evidence from Panel Data Analysis, Health Economics Review, 2, 22, 1-8.
- Raeesipour, A., Pazhouyan, J. (2013), The effect of government health spending on economic growth and Productivity in Iran: A regional approach, Planning and budgeting, Issue 4, Winter, 43-68.
- Rivera, B., Currais, L. (2004). Public health capital and productivity in the Spanish regions: A dynamic panel data model. World Development, 32(5), 871–885.
- Sarlak, A., kiyani, K. (2015), The impact health expenditure on economic growth in the country's, Iran Applied Economics Studies, Issue 31, Spring, 171-185.
- Spence, M., Lewise, M. (2009), Health and Growth, The International Bank for Reconstruction and Development, The World Bank.
- World Health Organization (2010), World Health Statistics; 2010.



