American Journal of Food Science and Health, Vol. 2, No. 5, October 2016 Publish Date: Aug. 19, 2016 Pages: 107-116
Management Perspectives of Food Safety and Poor Personal Health Management Among
Blue-Collar Workers in Nigeria
John N. N. Ugoani1, *, Margret. A. Ewuzie2
1College of Management and Social Sciences, Rhema University, Aba, Nigeria
2Department of Physical and Health Education, Alvan Ikoku Federal College of Education, Owerri, Nigeria
Abstract
The study was designed to explore the degree of relationship between food safety problems and personal health management among blue-collar workers, in Nigeria. The high rate of street foods patronage by blue-collar workers in Nigeria has given rise to the wide spread of food-borne diseases like staphylococcus aureus, streptococcus aureus, shigelia, and salmonella, among others. Itis believed that these type of diseases are strongly associated with poverty and in equality in society. On the other hand, there is strong and growing body of empirical evidence that higher social and economic status is associated with better health. The survey method was used for the study and it was found that the problems of food safety have strong positive relationship with poor personal health management among blue-collar workers in Nigeria.
Keywords
Food Security, Blue-Collar Workers, Staphylococcus Aureus, Streptococcus Aureus, Campylobacter Jejuni, Mama-Put,
Pure Water, Ngwongwo, Pepper-Soup, PHM
Received:July 13, 2016
Accepted: July 29, 2016
Published online: August 19, 2016
@ 2016 The Authors. Published by American Institute of Science. This Open Access article is under the CC BY license. http://creativecommons.org/licenses/by/4.0/
Contents
1. Introduction 1.1. Statement of the Problem 1.2. Objective of the Study 1.3. Scope of the Study 1.4. Significance of the Study 1.5. Limitations of the Study 1.6. Hypotheses 2. Literature Review 2.1. Food Safety and Health 2.2. Food Vending and Contamination 2.3. Major Common Food-Borne Diseases in Nigeria 3. Methodology 3.1. Participants 3.2. Materials 3.3. Procedure 3.4. Data Analyses 4. Presentation of Results 4.1. Discussion of Results 4.2. Scope for Further Research 4.3. Recommendations 5. Conclusion Biography
1. Introduction
Research has shown that in many countries clean water and food are not available for much of the population and millions die from water and food-borne diseases each year as a consequence (Bloom, 2007). The concept of a blue-collar worker describes those workers paid their wages on an hourly basis. This is contrary to a white-collar worker who performs job duties in offices and usually earnmonthly salaries. Blue-collar workers usually work with their hands as labourers, cleaners, maintenance assistants, artisans, truck – pushers, iron benders, brick-makers, among others. The terms "blue-collar worker" and "white collar worker" are occupational or job categorizations that attempt to distinguish workers who perform manual labour from those workers who perform professional jobs often in office environments. A typical feature of blue-collar worker is that he does not require formal education to perform the basic duties. Blue-collar workers are often unskilled and low-skilled people in society, and they earn lowly hourly wages. This status exposes them to poverty and inability to buy better foods, thereby rendering them vulnerable to various types of food-borne and water-borne diseases. To change the situation and save lives requires an equal chance at a healthy life. According to Cerrell (2007) with increased resources, improved policies, and greater political will, it is possible to transform health conditions in developing countries and save millions of lives. Personal health management (PHM) is used to describe self-management and continuous promotion of personal hygiene so as to put the individual in the driver’s seat of his or her health. Gee (2012) emphasizes that PHM is a continuous promotion of personal health responsibility; which provides people with access to timely actionable health information and key ingredients of empowerment that leads to greater self-efficacy. Health Canada (1996) states that personal health practices are the individual decisions people make that affect their health directly. These are behaviours people choose to do in their daily lives. Some examples are smoking, drinking alcohol, physical activity, and food choices. On the other hand, personal health practices and coping skills refer to those actions by which employees or individuals can take to cope with challenges and develop self-reliance, solve problems and make choices that enhance their health. Most common health problems have been found to relate to personal choices that are related to dietary or food habits. Personal dietary choices result to food safety and poor personal health management problemsamongblue-collar workers. According to Food and Agriculture Organization (1996) food safety is an integral part of food security and is defined as protecting the food supply from microbial, chemical and physical hazards that may occur during all the stages of food production, including growing, harvesting, processing, transporting, retailing and distribution. Food safety is a scientific discipline involved in the various ways of describing, handling, preparation, and storage of food that prevents food-borne illness. It is the assurances that food will not cause any harm to the consumer when it is prepared and eaten (WHO, 2007, Ewuzie, 2015). According to Ewuzie (2015) food security is sometimes confused with food security because the words security and safety are almost given the same meaning in many languages. Food security means ensuring that all members of a population have access to a supply of food in sufficient quantity and quality, regardless of their social or economic status. Ewuzie (2015) posits that food is a nutritive material which is eaten or drunk or absorbed for the growth and repair of life, nourishment, nutriment that increases, keeps active, and sustains the body. She asserts that a large quantity of food produced and distributed in Nigeria gets to the consumer in an unwholesome condition. Ewuzie (2015) believes that these factors promote rapid microbial infections and intoxication resulting in dietary inadequacy and food-borne diseases. There is growing evidence in the social science literature that health is not only a biomedical phenomenon, but also one that is influenced by social, psychological, cultural, economic and political factors of the people concerned, and these factors must be taken into consideration in defining and measuring health, in which case, health is both a biological and social phenomenon (Gerlach, 1999). This reflects the widely accepted definition of health by WHO (1948) that "Health is a state of complete physical, mental and social wellbeing and not merely an absence of disease or infirmity". This definition of health has the implication that moving toward a stateof optional health involves the individual making positive changes in dietary decisions. This approach puts the power and responsibility for personal health in the hands of the individual, and never the health nor regulatory authorities. Health Canada (1996) believes that developing positive lifestyle patterns helps in an improved personal physical, intellectual, social, occupational and spiritual growth and development of the individual in society. In a study Headike, et al (2012) using biological samples involving stool urine and fingernail content of 168 participants in Nigeria found most common food-borne diseases such as salmonella, shigella, campylobacter, Escherichia, staphylococcus aureusetc among food-handlers.
1.1. Statement of the Problem
Public Health Agency of Canada (1997) asserts that the contributions of human biology and health services to personal health are limited. It states that there are strong indications that other factors such as living and working conditions are crucially important for a healthy population. It believes that personal health practices and coping skills, healthy child development, biology and genetic endowment, health services, gender and culture, influence the state of personal health. According to Ewuzie (2015) food-borne disease is any disease or an infection of toxic nature caused, or thought to be caused, by the consumption of food or water. It can result from contamination with an extrinsic chemical or biological hazard associated with food. She opines that global incidence of food-borne diseases is very high. For example, The Centre for Disease Control and Prevention (CDCP) estimates show an annual occurrence of 478million food-borne illnesses in the US, 2 million in the UK, and 750,000 in France respectively. It is also estimated that in Austria, there are 5.4 million cases of food-borne illness every year causing 18,000 hospitalizations, 120 deaths, 21 million lost work days, 1.2 million doctor consultations and 300,000 prescriptions for antibiotics (USDA/DHHS, 2006, WHO, 2007, USDA, 2007). Even though such records are not well developed in Nigeria many lives are lost annually due to food-borne and water-borne diseases. In a study Ifeadike, et al (2012) using biological samples involving stool, urine and fingernail content of 168 participants in Nigeria, found most common food-borne diseases such as salmonella, shigella, campylobacter, escherichia, staphylococcus aureusetc among food-handlers. The Nigeria Factories Act (1987) as amended, in general provisions on health, makes it mandatory for employers to be responsible for the health, safety and welfare of employees in factories. According to Uvieghara (2001) every factory must be kept in a clean state and free from effluvia arising from any drain, sanitary convenience or nuisance. Accumulation of dirt and refuse must be removed daily by a suitable method from the floors and benches of workrooms and from the staircase and passages. Even though the government and employers are responsible for protecting workers from health and safety hazards, workers also have personal responsibility for protecting themselves by observing health and safety rules and regulations governing worker behavior. When people are healthy they are more productive, and in a better status to contribute to business success. Therefore, the challenge of common foodborne and waterborne bacterial pathogens and associated diseases must be confronted by both the health authorities and the management of organizations in Nigeria. A major objective of management at all levels is to ensure the stability, growth and profitability of enterprises and other institutions. To achieve the objective, management has to ensure that workers are free from diseases like campylobacter jejuni, clostridium botulimum, salmonella, streptococcus aureus, staphylococcus aureus, among others (USDA, 2008).
1.2. Objective of the Study
The study was designed to explore the relationship between food safety and poor personal health management problems among blue-collar workers in Nigeria.
1.3. Scope of the Study
The study was delimited to blue-collar workers in Nigeria.
1.4. Significance of the Study
The study will create awareness on the importance of food safety and personal health management among employees’, students, researchers, health authorities, and others interested in food safety and personal health management theory.
1.5. Limitations of the Study
The study was limited by the shortage of current relevant literature in the areas of interest. Lack of research funds also constrained the extension of the work beyond the South-East geopolitical zone of Nigeria.
1.6. Hypotheses
To achieve the object of the study, two hypotheses were formulated and tested at 0.05 level of significance.
Ho: There is no relationship between food safety and poor personal health management among blue-collar workers in Nigeria.
Hi: There is a relationship between food safety and poor personal health management among blue-collar workers in Nigeria.
2. Literature Review
Health is multidimensional, and WHO (1948) definition envisages three specific dimensions, the physical, the mental and the social. Others may include spiritual, emotional, vocational and political dimensions. Thus, personal health management is in this context used to describe a whole person approach that involves making positive attempts at cultivating lifestyle patterns that reflect an integrated movement towards a kind of equilibrium with factors like good dietary choices, income, social, education, employment or working conditions as well as the physical environment. The physical environment is an important determinant of health. At certain levels of exposure, contaminants in the air, water, food and soil can cause a variety of adverse health effects, including cancer, birth defects, respiratory illness and gastrointestinal ailments (Public Health Agency of Canada, 1997, Adedoyini, et al, 2006, Adeleke, 2009, Ajayi, et al, 2014, Annor and Baiden, 2011).
2.1. Food Safety and Health
In a biomedical conception, health is regarded as the absence of disease, therefore, if a person is free disease, then he or she is considered healthy. But other approaches to the understanding of the concept of health like the holistic proposal believes that all sectors of society have an effect on health, in particular, agriculture, industry, education, housing and food, among others (Canada Health, 1996). The holistic health approach has obvious implication for food safety. According to Ewuzie (2015) food safety has broad and considerable importance to public health. She states that living in today’s world has made health problems much more complicated than they were years ago partly due to more chemicals that individuals are exposed to through food consumption. Pollution, food additive, junk food, and other factors seem to have placed more burdens on health problems, leading to food-borne diseases that account for about 7.2million deaths annually, out of which about 80 percent are children (FAO, 2011, World Hunger Report, 2011). According to Ewuzie (2015) a national survey by the National Bureau of Statistics on food expenditure by states and commodity types showed that Nigeria spent over N110,320,796, on food as against N59,190,093, on none-food items like clothing, foot wear, rent, household goods, education, etc(NBS, 2007, Tolupe, et al, 2015, Onyeanacho and Hedberg, 2013, Ewuzie, 2004, FAO, 2013).
2.2. Food Vending and Contamination
Nigeria is polluted by the menace of foodvending. According Ewuzie (2015) food contamination may occur at any point during its journey through production, processing, distribution, and preparation. Food vendors have become an integral part of the food supply and consumption chain in Nigeria, mostly in the urban and semi urban areas. Today, street foods, as seen in bukas, are major sources of nourishment and enjoyment, as well as income for bothblue collar workers, and the urban poor. Street foods are sources of food-borne diseases, because they are at the risk of easy contamination. Ewuzie (2015) posits that street foods are usually stored at improper temperatures and sold from vending sites which include kiosks, make-shift accommodation, and push-carts, among others. This food vending phenomenon widely known as mama-put is popular among blue-collar workers in Nigeria, despite the fact that such foods are prepared at very dirty surroundings sometimes with waste water and garbages nearby, providing nutrient and breeding ground for microorganisms responsible for food-borne diseases (WHO, 2008) Okojie and Isah (2011) state that in Nigeria, urban city dwellers spend as much as half of their food expenditure on street foods. It is also believed that several food-borne diseases outbreaks are associated with poor personal hygiene, and practices of food vendors. (Adewunmi, et al, 2014, Monney, et al, 2013, Mekonnen, et al, 2012, MukhoPadhyay, et al, 2012, Osagbemi, et al, 2010, Osaili, et al, 2013, Ifeadike, et al, 2012)
2.3. Major Common Food-Borne Diseases in Nigeria
WHO (2000) identifies Salmonella and Campylobacter as the two most common causes of food poisoning throughout part of Europe, with more than 160,000 cases in 1999. It states that Salmonellosis is typically acquired from foods acting as vehicles of transmission. It is often characterized by an incubation period of 6.48 hours, followed by the onset of fever, headache, nausea, vomiting, abdominal pain and diarrhea. Other food-borne diseases include clostridium botulinum, escherichia, streptococcus aureus, staphylococcus aureus, among others. While streptococcus is often caused by poor personal hygiene, staphylococcus results from improper food handling. Shigelia is caused by food contamination and poor personal hygiene with the frequent symptoms of dysentery, fever, vomiting, diarrhea, among others (USDA, 2008, Chukwuezi, 2010, Chander, et al, 2013, Edwards, 2009, FAO, 2011, Fatirasun, et al, 2010, WHO, 2004). Chan (2015) while speaking in Abuja, Nigeria, states that as many as 600 million people in the world fall ill after consuming contaminated food. According to him, out of these millions of people, 420000 die including 125000 children under the age of five years. Chain (2015) opines that the burden of food-borne diseases is a public health concern globally, Africa and South-East Asia Regions now have the highest incidence and highest death rates, including among children under the age of five years, despite the fact that they make up only 9 percent of the global population. According to him most food-borne diseases are caused by 31 agents- bacteria, viruses, parasites, toxins and chemicals. In a study on the prevalence and pattern of bacteria and intestinal parasites among food handlers in the Federal Capital Territory of Nigeria, Ifeadike, et al (2012) observe that biological contaminants largely bacteria and other parasites constitute the major causes of food-borne diseases often transmitted through food, water, nails, and fingers contaminated with faeces. Accordingly food-handlers with poor personal hygiene could be potential sources of infections by these micro-organisms. They state that fingernail bacteria isolates include: E. Coli (1.8%) Coagulase-negative staphylococcus (17.9%), Staphylococcus aureus (7.1%), among others. Furthermore, 42.3 percent and 15.5 percent of the stool specimen of the 168 study population tested positive for salmonella and shigella species, respectively. Ifeadike et al (2012) insist that the consumption of contaminated or unsafe foods may result in illness, also referred to as food-borne disease. They contend that such diseases remain a major public health problem globally, but particularly in developing countries due to difficulties in securing optimal hygienic food handling practices. They estimate that about 70 percent of cases of diarrhoeal disease are associated with the consumption of contaminated food, even though reliable statistics on food-borne disease are not available due to poor or non-existent reporting systems in most developing countries. Ifeadike et al (2012) believe that the transmission of intestinal parasites and entero-pathogenic bacteria is effected through objects contaminated with faeces. These include food, water, fingernails, and fingers. On these bases, food-handlers with poor personal hygiene, who are working in food-providing entities, could be major potential sources of infections of many intestinal helminthes, protozoa, and entero-pathogenic bacteria. They find that compared to other parts of the hand, the area beneath fingernails harbours the most micro-organisms and is most difficult to clean. These researchers stress that, in developing countries biological contaminants are mostly responsible for a very wide range of diseases, including cholera, campylobacteriosis, E. Coli gastroenteritis, salmonellosis, shigellosis, typhoid and paratyphoid fevers, brucellosis among others. They emphasis that general good house-keeping, food handling preparation, serving practices, dishwashing facilities, conditions of cooking utensils, food storage systems, as well as food handlers knowledge and practices all affect food safety directly or indirectly. Contrary to this expectation, Ifeadike, et al (2012) report that 38.1 percent of the stool samples of the study population tested positive for A. lumbricoides, and 62.6 percent of the stool specimen tested positive for bacteria: Salmonella and shigella. This type of result would suggest that the promotion of personal hygiene among blue-collar workers and food handlers has become crucial in pursuing the UN objective of a healthy environment and the achievement of significant improvement in the lives of at least 100 million slum dwellers by the year 2020 (Alexandratos, 2005).
3. Methodology
3.1. Participants
The sample comprised of 300 participants, 200 males and 100 females ranging in age from 21 to 70 (M – 46 years, SD = 25). The participants were generated from the general population in South-East Nigeria.
3.2. Materials
A 5-point instrument titled Food Safety Questionnaire (FSQ) and based on the Likertscale, ranging from "5 = strongly agree to "1 = strongly disagree was used to generate data. The Likert scale has previously been validated and is commonly used for attitude measurement (Nworuh, 2004).
3.3. Procedure
The questionnaire copies were personally administered on the respondents by the investigator and two research assistants. Respondents were simultaneously subjected to oral interviews so as to supplement, complement and validate data through each other. All the materials were retrieved and the responses found useful for analyses.
3.4. Data Analyses
Data were analyzed through descriptive and Chi-Square statistical methods. Chi-Square statistics is amenable to a wide spectrum of data especially those used on the nominal, ordinal, internal, or ratio scales, which are tallied as individual responses (Nworuh, 2004). The results were presented in tables.
4. Presentation of Results
Table 1. Common food-borne bacterial pathogens and associated diseases.
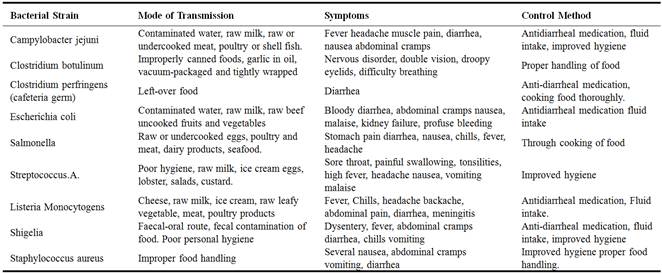
Source: USDA (2008) Food-Borne Illness: What consumers need to know.http://www.fsis.usda.gov/factsheets.
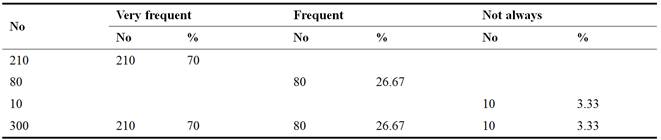
Table 2. Consumption of garri in bukas.
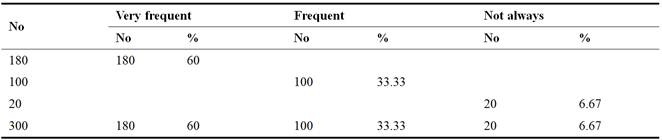
Source: Field work, 2016
Garri is a by-product of cassava consumed in very high frequency by Nigerians in many roadside eating places popularly called "Bukas"
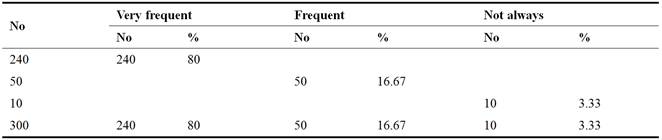
Table 3. Consumption of pepper soup.
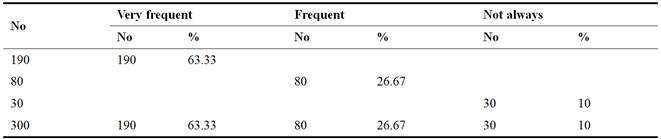
Source: Field work, 2016
Table 3 showed that about 63 percent of blue-collar workers very frequently patronize pepper soup spots scattered in many unhygienic environments in both urban and semi urban towns in Nigeria.
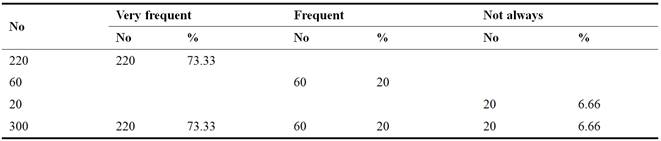
Table 4. Consumption of sachet water.
Source: Field work, 2016.
Table 4 proved that about 70 percent of blue-collar workers drink sachet water, popularly known as "pure water" that is usually produced from borehole water. This could be a major source of water-borne diseases.
Table 5. Consumption of bush meat.
Source: Field work, 2016
Analysis in table 5 showed that about 73 percent of blue-collar workers among Nigerians eat bush meat, in most cases hawked about at motor parks, etc. thereby rendering themselves vulnerable to various types of food-borne diseases.
Table 6. Consumption of Ngwongwo.
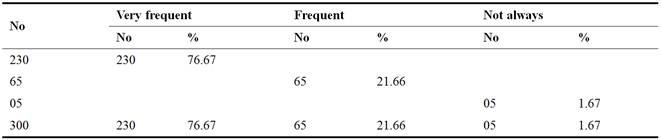
Source: Field work, 2016
Table 6 confirmed the assumption that over 76 percent of Nigerians enjoy eating a delicacy called "Ngwongwo" which is a mixture of different meat parts with some vegetables and spices. Many blue-collar workers hardly miss a day without enjoying ngwongwo.
Table 7. Consumption of local gin.
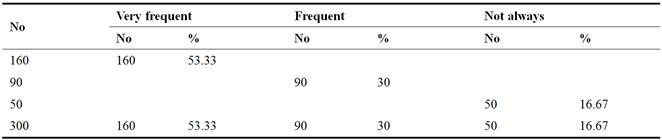
Source: Field work, 2016
Table 7 suggested that more than 50 percent of Nigerian low income earners consume local gin popularly known as "ogogoro," sometimes mixed with other chemicals.
Table 8. Patronage of mama-put.
Source: Field work, 2016
The percentage of people who patronize "mama-put" as in table 8, which is used to describe cooked food items sold by poor women on push carts supports the evidence in literature that many Nigerians eat street foods. Mama-put has become a popular food supply chain that even some white-collar workers buy for consumption in their offices and homes.
Table 9. Environments of street foods.
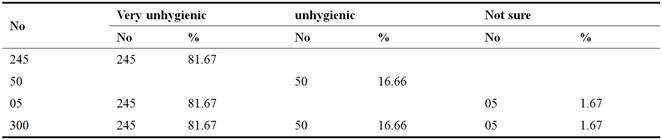
Source: Field work, 2016
Table 9 showed that over 81 percent of respondents believe that the environments of street foods in Nigeria are very unhygienic. These foods are often cooked under leaking roofs, with garbage heaps around. This clearly supports the study of Ifeadike et al (2012) that food handlers with poor personal hygiene could be the major causes of food-borne diseases in Nigeria.
Table 10. Test Statistics.

Source: X2 Analysis
4.1. Discussion of Results
Bloom (2007) suggests that some diseases are strongly associated with poverty and in equality in society. In many developing countries like Nigeria blue-collar workers, very frequently patronize street foods. There is also strong and growing evidence that higher social and economic status is associated with better health. However blue collar workers mostly fall within the poverty levels in society and can hardly afford better foods than to patronize street foods when they are not at home, thereby rendering themselves vulnerable to food-borne and water-borne diseases. In Nigeria today, it is common to have traditional medicine men and women boarding commercial buses plying the major cities to advertise and sell local herbs and roots for the treatment of streptococcusaureus, staphylococcus aureus, escherichia coli, shigelia, salmonella, among others. The high rate at which the unrefined trado-medicinal items are patronized by the majority of travellers and others for the possible treatment of these diseases would suggest that they have become widespread in Nigeria. Also, common symptoms of health problems among blue-collar workers in Nigeria have often been fever, headache, muscle pain, vomiting diarrhea, dysentery, tonsillitis, sore throat, among others, that are associated with common food-borne bacterial pathogens and associated diseases, as described in table 1 (USDA, 2008). The phenomenon of these diseases in Nigeria cannot be over emphasized, bearing in mind the high illiteracy level and the fact that about 70 percent of the general populations are poor. Social status is a vital component in an individual’s personal capacity to effectively negotiate societal systems. Health Canada (1996) suggests thathealth status improves at each step up the income and social hierarchy. It insists that adequate income ensures that basic living conditions are met, such as access to safe housing, and the capacity for the maintenance of health. According to Health Canada (1996) there is a large body of empirical evidence which links poverty to a shorter life expectancy and higher socio-economicstatus to a slower progression of disease. The case of the blue-collar workers in Nigeria is the case of the poorest of the poor that do not have the capacity to buy sufficient good food needed for better health status. As in table 2, about 60 percent of blue-collar workers eat garri prepared under mostly unhygienic conditions at bukas, thereby facing the chances of having staphylococcus aureus. Pepper soup consumption at local restaurants is common among blue-collar workers in Nigeria, and because of poor hygiene, consumers are prone to streptococcus aureus. High rate of consumption of sachet water, popularly called purewater, bushmeat, and popular local delicacy called ‘Ngwongwo’ renders consumers vulnerable to escherichia coli, among others. The consumption rate of local gin, mixed with other chemicals is wide spread among blue-collar workers. They can afford to forego food but never to forgo drinking "ogogoro". The patronage of "mama-put", the food sold by poor women on push carts, usually prepared in unhygienic environments give rise to the high rates of fever, headache, diarrhea, stomach pain, among blue-collar workers. The test statistic in table 10 showed that the Chi-Square value of approximately 31 was greater than the table value of approximately 9, at 0.05 level of significance and with 4 degrees, of freedom. This technically means that the problems of food safety have significant positive relationship with poor personal health management among blue-collar workers in Nigeria. To this extent Ho: was rejected, while the alternate was accepted. This is the crux of the study. This result supports the strong views of Health Canada (1996), Bloom (2007) Ifeadike, et al (2012) among others that food-borne diseases are strongly associated with poverty, in-equality, low social status and food handlers with poor personal hygiene.
4.2. Scope for Further Research
Further study should examine the role of government in regulating the promotion of local herbs as treatment for food-borne diseases to avoid causing more harm to consumers.
4.3. Recommendations
i) Governments at federal and state levels should make proper regulation for the control of street foods in Nigeria. This is important to safeguard the health of the poor numerous consumers.
ii) Consumers of street foods need to apply personal hygiene like ensuring that they use clean materials during consumption. This will reduce the rate at which they are infected by food-borne diseases.
iii) Consumption of local gin, known as "ogogoro" is rampant in Nigeria. The National Drug Law Enforcement Agency (NDLEA) should wake up to its duties and ensure that dangerous chemicals are not used in its production, because of the level of intoxication observed among consumers.
iv) Bukas keepers need to prepare their foods in clean environments. The present situation where this is done beside heaps of waste, with dirty water, leaking roofs help greatly to contaminate the foods.
v) The regulation of the production of sachet water should be strengthened to guarantee the safety of the numerous drinkers. Some of the sachet waters that is said to have the approval of National Agency for Food, Drugs, Administration and Control (NAFDAC) still have some taste. This could mean improper treatment and such waters may lead to serious water-borne diseases like campylobacter jejuni and Escherichia coli, among consumers.
5. Conclusion
High rate of consumption of street foods often prepared under unhygienic conditions by blue-collar workers renderthem vulnerable to food-borne and water-borne diseases such as staphylococcus aureus, streptococcus aureus, campylobacter jejumi, escherichia coli, salmonella, among others. The rate of hawking local herbs and roots for the possible treatment of these diseases, and the patronage by blue-collar workers go to confirm that such diseases have become rampant. The evidence that these diseases are strongly associated with poverty, inequality, and low social status and food handlers with poor personal hygiene suggests that the consumers of street foods are trapped because of their inability to buy better foods and water. In contribution to previous research on food safety and personal health management, this study found strong positive relationship between problems of food safety and poor personal health management among blue-collar workers in Nigeria. This is the interest of the study, and it supports the previous works of Ewuzie (2015) Ifeadike, et al (2012) among others that many Nigerians are infected by various food-borne and water-borne diseases.
References
- Adedoyini, O. T, Ojuawo, A., Adesiyun, O. O., Mark, F. Anigilaje, E. A (2006).Poisoning due to yam flour consumption in five families in Ilorin, Central Nigeria, West Afr. Med. J. 27, 41-43.
- Adeleke, S.I, (2009).Food poisoning due to yam flour consumption in Kano (North West). Nigeria online J. Health Allied Scs, 8, (10), 10-14.
- Adewunmi, A. R., Ajayi, J. O and Omotoso, B. O. A (2014) Assessment of the Hygiene Practices of Food Vendors and Government Intervention in Selected Secondary School from Abeokuta South Local Government Area of Ogun State, Nigeria. Journal of Science and Multidisciplinary Research. 6(1), 70-78.
- Ajayi, O. A, Oluwoye, J. and Williams, L. L (2014) Policy options on Reduction of Food Borne Diseases. Food and Public Health 4(6) 266-271.
- Alexandratos, N. (2005) Countries with rapid population growth and resource constraints. Issues of foods, agriculture, and development. Population Development Review, 2005:31-237-258. The World Bank, Washington, D.C.
- Annor, G. A, Baiden, E. A (2011).Evaluation of Food Hygiene Knowledge, Attitudes and Practices of Food Handlers in Food Businesses in Accra, Ghana. Food and Nutrition, 2:830-836.
- Bloom, D. E. (2007) Governing Global Health.Finance and Development. Vol. 44, No. 4, pp. 31-35.
- Cerrell, J. (2007) Is the Global Health System Broken? Finance and Development. Vol. 44, no. 4, pp: 36-38.
- Chan, M, (2015) Nigeria: Food-Borne Diseases 600 Million Affected Annually – WHO. Leadership, Abuja, 4 December 2015.
- Chander, P. T., Rakesh, M, Chahat, N., Swati, M, and Tapan, J. K (2013).Food Safety and Hygiene Practices among street food vendors in Delhi, India.International Journal of Current Research 5 (II) 3531-3534.
- Chukwuezi, C. O (2010) Food Safety Hygiene Practices of Street Food Vendors in Owerri, Nigeria. Studies in Sociology of Science (Cc) 50-57.
- Edwards, E. (2009) Food Safety – The Nigerian Experience.Retrieved from http://www.slideshare.net/worldtap/food safety Nigeria.
- Ewuzie, M. A (2004) Perspective on Human Nutrition.Owerri, Nigeria, Cherry Bren & Co. 184-202.
- Ewuzie, M. A (2015) Food Safety and Health: A Review of Literature, A Paper Presented at the 20th Annual Conference of the Nigerian Association of Health Educators (NAHE) at the Faculty of Education, Main Auditorium, University of Ilorin From 22nd – 25th July, 2015.
- FAO, (2013) National Food Control System in Africa; A Situation Analysis, a Presented at the FAO/WHO Regional Conferences on Food Safety for Africa, Harare, Zimbabwe, Accra Food and Agriculture Organization, Regional Office for Africa.
- FAO, Report of the World Food Summit, Rome, 13-17 Nov. 1996, Food and Agriculture Organization.1996, http://www.fao.org/dorep/003/w3548e/w3548e000.htm, accessed 17 Nov. 2006.
- FAO/WHO Regional Conference on Food Safety for Africa (2005) Informal Food Distribution Sector in Africa (Street Foods): Importance and Changes.
- FAO (2011) World Hunger Report: High Volatile Price set to Continue. Available on Line: http://www.fao/news/story/en/item/92495/icode/. Retrieved April 29th, 2014.
- Fatiregun, A. A., Oyebade, O. A, Oladokun, L. (2010) Investigation of an out Break of Food Poisoning in a resource – limited setting. Trop. J. Health Sci. 17, 117-4153.
- Federal Republic of Nigeria Factories, Act (1987).
- Gee, T. (2012) Personal Health Management (PHM): Singapore’s National Strategy to Activate and Empower Patients and Care Givers Through Innovative Personal Technologies. International Journal of Integrated Care, Volume 12, 15 June 2012.
- Gerlach, J (1999) The Continuing Problem of Extra Pyramidal Symptoms. Strategies for Avoidance and Effective Treatment. J Clin Psychiatry 1999; 60 (23); 20-24.
- Health Canada (1997).Health and Environment Ministry of Health and Environment Series.http://www.hc-sc.gl.ca
- Health Canada (1996)Health and Environment Ministry of Health and Environment Series.http://www.hc-sc.gl.ca
- Ifeadike, C. O, Ironkwe, O. C, Adogu, P. Nnebue,, C. C, Emelumadu, O. F, Nwabueze, S. A, and Ubajaka, C. F (2012) Prevalence and pattern of bacteria and intestinal parasites among food handlers in the Federal Capital Territory of Nigeria.Nigerian Medical Journal 2012, 53.166-71.
- Monney, I., Ageyi, D. and Owusu, W. (2013) Hygiene Practices among Food Vendors in Educational Institutions in Ghana: The case of Konongo Foods, 2, 282-294, www.mdpi.com/journal/foods
- Mekonnen, H. Habtamu, T., &Kelali, A (2012) Source (s) of contamination of "raw" and ready of eat foods and their public health risks in Mekelle City Ethiopia, ISABB Journal of Food and Agricultural Science vol. 2(2).
- Mukhopadhyay, P. Joardargk, Bag.K., Samanta, A, Sain, S., Koley, S. (2012). Identifying Key Risk Behaviour, Regarding Personnel Hygiene and Food Safety Practices of Food Handlers Working in Eating Establishments Located within a Hospital Campus in Kolkata. Al Ameen J. Med. Sci, 50:21-28.
- National Bureau of Statistics (2007) Abuja.
- Okojie, P. W and E. C Isah. (2014) Sanitary Conditions of Food Vending Sites and Food Handling Practices of Street Food Vendors in Benin City, Nigeria: Implication for Food Hygiene and Safety. Hindawi Publishing Corporation Journal of Environmental and Public Health.
- Osagbemi, G., Abdullahi, A., Aderibigbe, S. (2010). Knowledge, Attitude and Practice Concerning Food Poisoning Among Residents of Okene Metropolis, Nigeria Res. J. Soc. 1, 61-64.
- Osaili, T. M, Abu Jamous, D. O., Obeidat, B.A; Bawadi, H. A Taggem, R. F.; Subih H. S (2013) Food Safety Knowledge Among Food Workers in Restaurants in Journal. 31, 145-150.
- Public Health Agency of Canada (1997) Available at http://www.publichealth.gc.ca Retrieved 28/5/15.
- Public Health Act, (2012). Act 851, Available online. FAO level. Fao.org/docs/pdf/gha136559.pdf (Date accessed 24/10/2014).
- Sylvester, N. Onyenacho and Craig W. Hedberg (2013). An Assessment of Food Safety Needs of Restaurants in Owerri, Imo State, Nigeria. International Journal of Environmental Research and Public Health 10, 3296-3309.
- Tolupe, O. A. Zuwaria, H, Danjuma, A. & Bello Z. (2015) Knowledge and Practices of Food Safety and Hygiene among Food Vendors in Primary Schools in Jos, Plateau State, North Central Nigeria. E3 Journal of Medicines Research, vol. 4 (2).
- USDA/DHHS (Us Department of Agriculture and US Department of Health and Human Services) (2006).Nutrition and your health. Dictionary Guidelines for America’s (5thed) USDA Home and Garden Bulletin No. 232 Washington DC US Government Printing Office.
- USDA (2007).Food Safety and Inspection Service Pearson Education Inc. USDA.
- USDA (2008). Food-Borne Illness: What Consumers Need to Know: http://www.fsis.usda.gov/factsheets
- Unieghara, E. E (2001) Health, Safety and Welfare in Factories. In E. E Uvieghara (ed) Labour Law in Nigeria. Lagos, Malthouse Press Ltd pp: 193.
- World Health Organization (1948) Constitution USA.
- World Health Organization (WHO) (2004). Food and Health in Europe: a new-basis for action. WHO Regional Publications European Series, No. 96 pg 91-93.
- World Health Organization (WHO) (2004). World Health Organization Global Strategy for Food Safety: Safer Food for Better Health; Available from: http://www.who.int/fooodsafety//publications/general/enstrategy-pdf. (Last accessed on 2014 May, 30).
- World Health Organization (WHO) (2007). Food Safety and Health: A Strategy for the WHO African Region.
Biography
|
|
|
|





