International Journal of Environmental Planning and Management, Vol. 1, No. 2, June 2015 Publish Date: May 6, 2015 Pages: 33-40
Assessment and Characterization of Hospital Waste in Government and Private Hospitals of Rawalpindi City
Madhia Aslam1, Syed Atif Shaukat2, *, Audil Rashid1, Azeem Khalid1, Syed Kashif Shaukat3, Syed Waasif Shoukat4
1Department of Environmental Sciences, PMAS Arid Agriculture University, Rawalpindi, Pakistan
2Govternment Boys High School Bangoin Rawalakot, Poonch, Education Department, Azad Jammu & Kashmir, Pakistan
3Department of Soil & Environmental Sciences, Faculty of Agriculture Rawalakot, University of Azad Jammu & Kashmir, Pakistan
4Department of Environmental Sciences, Islamic International University Islamabad, Pakistan
Abstract
Hospital waste management is a growing environmental concern in developing countries. Rawalpindi, is among the big cities of Pakistan which has population over four million and generates large quantities of waste. Many efforts have been made by environmental regulatory agencies and waste generators to better managing the wastes from healthcare facilities in recent years. To better manage, characterization and continuous assessment of hospital waste is essential. With this aim a comparative study was carried out in 34 different hospitals of Rawalpindi. The goals of this study were to characterize the solid waste generated in the hospitals, to provide the current status of waste management and to provide the framework for the safe management of waste in the surveyed hospitals. For this purpose a Questionnaire survey was conducted to gather information about waste handling, safety measures and overall awareness among hospital staff. Type of the hospital was significantly associated with various factors such as total number of beds, number of inpatients, outpatients and total waste generation. A predominantly significant correlation (r = 0.67, P<0.001) between rate of waste generation and number of occupied beds was observed in government hospitals. Results of hospital waste characterization show that 25–35% waste comprises of infectious waste in almost 42.5 % of all hospitals. More than 50% hospitals practiced separation of risk and non-risk waste. Incineration was mostly used as hazardous waste disposal option in the surveyed hospitals (97.5%). The study depicted better conditions in government hospitals as compared to private hospitals such as point segregation and use of colored containers for specific waste type(P<0.05). In term of protective clothing and training facilities to waste handlers, government hospitals had better status. It is recommended that for efficient waste management there is need to improve the training of waste handlers and source separation of the waste.
Keywords
Comparison, Contamination, Environment, Segregation, Incineration, Waste Management
Received: April 3 2015 / Accepted: April 15 2015 / Published online: May 5, 2015
@ 2015 The Authors. Published by American Institute of Science. This Open Access article is under the CC BY-NC license. http://creativecommons.org/licenses/by-nc/4.0/
Contents
1. Introduction 2. Materials and Methods 2.1. Sampling Sites 2.2. Sampling 2.3. Questionnaire Survey 2.4. Statistical Analysis 3. Results 3.1. Waste Generation and Characterization 3.2. Waste Collection and Segregation 3.3. Waste Storage 3.4. Waste Treatment and Disposal 3.5. Training and Protection of Waste Handlers 4. Discussion 5. Conclusion
1. Introduction
As the societies are becoming more modern everything (material, objects, and devices) is becoming waste. The amount of waste is increasing constantly due to increase in population and population density and with the industrial and economic advancements which disrupt the natural equilibrium and creates economic, ecological and health problems for society (Askarian et al., 2004; Marinkovic et al., 2008). Environment is facing severe problems due to unsustainable waste disposal due to which environmental and natural resources can be polluted and human beings animals and plants can be impacted (Sabour at al., 2007). It is a sensitive issue which concerns about serious environmental problems in today’s world. Domestic industrial and other wastes whether they are of low or medium level wastes are causing environmental pollution and have become persistent problem for mankind (Ramasamy et al., 2008).
Hospital waste management is a vital public health and environmental issue. There has been an increased public concern about the management of healthcare waste during the past few years on a global basis (Shinee et al. 2008). HW is the special category of waste because it possesses potential health and environmental risks (Beveja et al. 2002). Pathological, infectious, chemical, pharmaceutical and sharps contaminated with blood, infectious agents, tissues, and organs are some of the important constituents of hospital waste (Alagoz and Kocasoy, 2008). Compare to municipal solid waste, 75-90% of hospital waste is referred to as non-risk or general waste while the remaining 10-25% is regarded as infectious and hazardous and may create variety of health risks (Chaerul et al. 2008). The increased amount of waste is attributable to hospital size, services they provide along with the increased medical disposable products (Mohee, 2005). The composition of waste differs from one hospital to another depending upon the economic and cultural status of the patients and condition of that area where the hospital is located (Askarian et al. 2004). Hospital waste management is a critical public health and environmental issue (Ruoyan et al. 2010). Improper waste management can cause environmental pollution, unpleasant odors, and growth of insects, rodents and worms; it may lead to transmission of diseases like typhoid, cholera, and hepatitis through injuries from sharps contaminated with human blood (Abdullah et al. 2008). In order to set up a proper hospital waste management system, many factors including public health, economic status, social aspects, regulations, hospital management, etc. need to be incorporated into the system and it is essential to determine all of the interactions among those factors (Chaerul et al., 2008). It is of great importance to manage medical waste in a proper manner to avoid health risks and damage to flora, fauna, and the environment.
Many management systems and practices are available for the appropriate handling and safe disposal of hospital waste such as landfill, incineration, autoclaving, and recycling (Li et al., 2002; Plenik and Cumberland., 1993).
Developing countries face severe problem in managing their waste because segregation of waste does not takes place properly and in most of the developing countries hospital waste is still handled and disposed of together with domestic waste and creates great threat to public health and environment (Silva et al., 2005; Diaz et al., 2008). In the hospitals of Rawalpindi city waste is not collected separately and there is no control of mixing infectious and non-infectious waste. In this context the proposed work is aimed at exploring the current status of hospital waste management including handling, treatment, final disposal and total waste generation in Rawalpindi city. In addition to examine medical staff member’s knowledge of waste management policy and to understand protective measures regarding occupational safety.
2. Materials and Methods
A comparative two phase study was designed. In the first phase of the study sampling of waste has been carried out and in the second phase questionnaire survey was conducted.
2.1. Sampling Sites
Total 34 hospitals were selected. Twenty were government and 14 were private hospitals.
2.2. Sampling
The purpose of the sampling was to collect data about waste generation its composition and characteristics. For waste characterization, generated wastes (hazardous waste and general wastes) were weighed separately on suspension spring scale. For composition determination hospital waste it was sorted, into pharmaceutical waste, radioactive waste, sharps and pathological waste. These categories were weighed separately and the results were recorded. The method used for sampling was according to the method used by Taghipour et al., 2008.
2.3. Questionnaire Survey
In the second phase of the study a questionnaire related to collection, handling treatment and disposal of hospital waste was used. Design of questionnaire was in accordance with Birpinar et al. (2009) and Coker et al. (2009). The aspects included in the survey were: collection method, safety measures, awareness, collection frequency, satisfaction level of the respondents from waste management.
2.4. Statistical Analysis
Data collected from the sampling and survey was analyzed by using Microsoft Excel and SPSS. Chi square analysis was used to find out the association among waste generation and different parameters i.e. total number of beds, total number of inpatients and total number of outpatients in MS Excel. Correlation between number of beds and total amount of waste generated was found using SPSS package for windows.
At the end of the statistical data analysis which was performed use to determine that how much waste is generated in the surveyed hospitals of Rawalpindi city. Moreover the following results have also been used to find out what sorts of measures are required to reduce the solid waste generation.
3. Results
3.1. Waste Generation and Characterization
The percentage of general waste, pathological waste, radioactive waste, sharps and pharmaceutical waste are presented in Figure 1. General waste was observed higher in government hospitals (75%) as compared to the private hospitals (35%). Contrary to this sharps and pharmaceuticals were found higher in private hospitals.
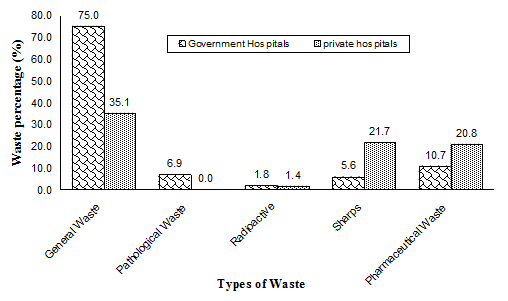
Figure 1. Waste characterization summary for Government and Private Hospitals (n=40)
Table 1. Characteristics of patients and hospital waste generation in the private and government hospitals from Rawalpindi city.
| Variable | Type of hospital | *Chi–square | P–value | |||
| Private (n = 20) | Government (n =14) | Total (n=34) | ||||
| n(%) | n(%) | n(%) | ||||
| Total number of beds | ||||||
| <150 | 20(100) | 0(0) | 20(50.0) | 40.00 | <0.005 | |
| 600-1200 | 0(0) | 14(100) | 14(50.0) | |||
| Number of inpatients | ||||||
| <100 | 20(100) | 0(0) | 20(50.0) | 40.00 | <0.005 | |
| >450 | 0(0) | 8(60) | 8(30.0) | |||
| <850 | 0(0) | 6(40) | 6(20.0) | |||
| Number of outpatients | ||||||
| <100 | 0(0) | 7(50) | 7(25) | 19.25 | <0.005 | |
| 150-300 | 20(100) | 5(35) | 25(67.5) | |||
| 850-1200 | 0(0) | 2(15) | 2(7.5) | |||
| Total waste generation | ||||||
| <100kg/d | 20(100) | 1(5) | 21(52.5) | 36.19 | <0.005 | |
| 1000-1200 kg/d | 0(0) | 9(65) | 9(32.5) | |||
| 1200-1600 kg/d | 0(0) | 4(30) | 4(15.0) | |||
A significant association of hospital type with waste generation, total number of beds and total number of inpatients and outpatients was tabulate through Chi-square (Table 1).
As the study was conducted in thirty four different hospitals of Rawalpindi city interesting correlation results were observed between total number of beds and amount of waste generated. In government hospital correlation between number of beds and waste generation was observed significantly positive (r= 0.67, p<0.0005) which was also clearly visible in scatter diagram (Figure 2).
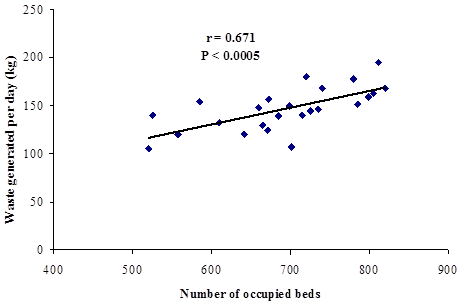
Figure 2. Relationship between number of occupied beds and waste generation in government hospitals Rawalpindi from February 2009 to July 2010.
3.2. Waste Collection and Segregation
Waste collection and segregation practiced by the private and government hospitals of Rawalpindi city is presented in Table 2. The results showed that among all the surveyed hospitals 95 % hospitals collect there waste in containers and remaining 5% hospitals use plastic bags for waste collection. Source segregation of hazardous and non-hazardous waste is practiced by 80% of the surveyed population with separate storage options for these two types of waste. The use of different containers for waste collection was significantly higher in government hospitals as compared to private hospitals (χ2=15.78, P<0.001). Similarly waste segregation practices was more notable in government hospitals then the private hospitals (χ2=10.00, P<0.002). For segregation color coded bags / containers and labeling of color coded bags was observed in most of the surveyed hospitals during site visits. The results revealed that 22.5 percent of the surveyed hospitals do not used any color coded bags/ containers for segregated waste, while in 77.5 percent of the hospitals color coded bags/containers were labeled at segregation time with proper biohazard symbols (Table 2).
3.3. Waste Storage
Once the waste is generated, it is usually collected and transferred to the temporary waste storage area by the hospital staff. The results showed that 87.5 % of the surveyed hospitals have temporary waste storage room (Table 3). In 57.5% of the total hospitals the proportion of infectious waste generated was 10-25 % of the total waste however, in 42.5 % of the surveyed hospitals fraction of infectious waste generated was 25-35 % per day of the total waste. Separate storage of risk and non-risk waste was observed in 77.5 % of the surveyed hospitals. Storage time for the risk waste was observed 12-24hrs in 90 % of the surveyed hospitals (Table 2).
3.4. Waste Treatment and Disposal
Table 3 shows the common practices used for treatment and disposal of hazardous waste. About 97.5 percent of the surveyed facilities disposed of their hazardous waste using incinerator. In addition to incineration, there are some other methods practiced in Rawalpindi for disposing of different types of hospital hazardous waste. Open dumping was practiced by about 37.5 percent of the hospitals (Table 3).
3.5. Training and Protection of Waste Handlers
The data about the training and protection of waste handlers indicated that government hospitals comply safety protocol of immunization for waste handlers better as compared to private hospitals since the higher Percentage of compliance was observed higher in government hospitals then the private hospitals (χ2=8.64, P<0.003) (Table 3). Lack of waste management team was found in 30% of the hospitals and the proportion of waste management team was significantly higher in government hospital then the private hospital (χ2=3.58, P<0.002). Information obtained from Questionnaire survey revealed that in 85% of the hospitals the waste handlers use protective clothing’s (Table 3). Training deficit to the waste handling staff was observed in 30% of hospitals.
Table 2. Characteristics of waste segregation, collection and storage in the private and government hospitals from Rawalpindi city.
| Variable | Type of hospital | Chi-square | P–value | |||
| Private (n = 20) n(%) | Government (n = 14) n(%) | Total (n=34) n(%) | ||||
| Waste is collected in containers | ||||||
| No | 2 (10) | 0 (0) | 2(5) | 2.10 | N-S* | |
| Yes | 18 (90) | 14 (100) | 32(95) | |||
| Type of containers to collect waste | ||||||
| Plastic | 16(80) | 7(50) | 23(65) | 15.38 | 0.000 | |
| Metal | 0(0) | 7(50) | 7(25) | |||
| Plastic bags | 4(20) | 0(0) | 4(10) | |||
| Waste segregation at source point | ||||||
| No | 8 (40) | 0 (0) | 8(20) | 10.00 | 0.002 | |
| Yes | 12 (60) | 14(100) | 26(80) | |||
| Color coding for segregation | ||||||
| No | 4 (20) | 9(70) | 13 (45) | 10.28 | N-S | |
| Yes | 16 (80) | 5 (30) | 21(55.0) | |||
| Biohazard Labeling of color coded bags | ||||||
| No | 6 (30) | 2 (15) | 8(22.5) | 1.29 | N-S | |
| Yes | 14 (70) | 12 (85) | 26(77.5) | |||
| Who handles the segregated waste | ||||||
| Hospital staff | 20(100) | 12 (90) | 32(95) | 2.10 | N-S | |
| Other | 0(0) | 2 (10) | 2(5) | |||
| Waste handlers satisfied with the salary | ||||||
| No | 11 (55) | 10 (75) | 21(65) | 1.75 | N-S | |
| Yes | 9 (45) | 4 (25) | 13(35) | |||
| Storage facility for waste | ||||||
| No | 3(15) | 1(10) | 4(12.5) | 0.22 | N-S | |
| Yes | 17 (85) | 13(90) | 30(87.5) | |||
| Risk and non-risk waste stored separately | ||||||
| No | 7(30) | 1(10) | 8(22.5) | 3.58 | 0.002 | |
| Yes | 13(65) | 13(90) | 26(77.5) | |||
| Proportion of infectious waste generated per day | ||||||
| 10-25% | 9(45) | 10(70) | 19(57.5) | 2.55 | N-S | |
| 25-35% | 11 (55) | 3 (30) | 14(42.5) | |||
| Proportion of infectious waste generated per day | ||||||
| 10-25% | 9(45) | 10(70) | 19(57.5) | 2.55 | N-S | |
| 25-35% | 11 (55) | 3 (30) | 14(42.5) | |||
| Maximum storage time for infectious waste in hospital | ||||||
| 12-24hrs | 18(90) | 12(90) | 30(90) | 0.00 | N-S | |
| 24-36hrs | 2(10.0) | 2(10) | 4(10.0) | |||
* N-S – non significant
Table 3. Comparison of some selected features related to training and management of hospital wastes in private and government hospitals of Rawalpindi city.
| Variable | Type of hospital | Chi-square | P–value | ||
| Private (n = 20) n(%) | Govt. (n = 14) n(%) | Total (n=34) n(%) | |||
| Does hospital has waste management team? | |||||
| No | 7(35) | 2(10) | 9(30.0) | 3.58 | 0.002 |
| Yes | 13(65) | 12(90) | 25(70.0) | ||
| Immunization protocol followed for waste handlers | |||||
| No | 12(60) | 2(15) | 14(37.5) | 8.64 | 0.003 |
| Yes | 8(40) | 12(85) | 20(65.5) | ||
| Handlers use protective clothing | |||||
| No | 3 (15) | 2 (15) | 5(15) | 0.00 | N-S |
| Yes | 17 (85) | 12 (85) | 29(85) | ||
| Satisfied with waste management in your hospital | |||||
| No | 12(60) | 1(5) | 13(32.5) | 13.78 | 0.000 |
| Yes | 8(40) | 13(95) | 21(67.5) | ||
| Plan for waste transportation | |||||
| No | 15(75) | 2(15) | 17(45) | 14.54 | 0.000 |
| Yes | 5(25) | 12(85) | 17(55) | ||
| Weighing of hospital waste before final disposal | |||||
| No | 11(55) | 7(50) | 18(52.5) | 0.10 | 0.002 |
| Yes | 9(45) | 7(50) | 16(47.5) | ||
| Training facilities available for waste management | |||||
| No | 6(30) | 4(30) | 10(30.0) | 0.00 | N-S |
| Yes | 14(70) | 10(70) | 24(70.0) | ||
| Final disposal for infectious waste | |||||
| Incineration | 20(10) | 13(95) | 33(97.5) | 1.02 | N-S |
| Municipality | 0(0) | 1(5) | 1(2.5) | ||
| Final disposal option for non-infectious waste | |||||
| Open dumping | 13(65) | 2(10) | 15(37.5) | 13.23 | N-S |
| Landfill | 0(0) | 1(5) | 1(2.5) | ||
| Others | 7(35) | 11(85) | 24(60) | ||
4. Discussion
Proper hospital waste management is greatly related to the reliable information of waste generation and type (Yong et al., 2009). Usually a number of factors effect the composition of waste and these factors include number of patients, number of beds, type of health services provided economic, social and cultural status of the patient and waste segregation system (Tudor et al., 2005). It is generally assumed that quantitative increase in any one of these variables would cause an increase in waste generation rate. Result of the current study have specifically pointed out an overwhelming evidence in favors of the existing relationship among similar sort of parameters. For instance out of forty selected hospitals of Rawalpindi city in government hospitals a significantly positive correlation was observed for total number of beds and waste generation. The reason behind is that the government hospitals large number of visitors to the patients increase the non-risk waste in form of food items and refuses. Sanida et al., 2010 used linear correlation to examine the relationship between waste generation and number of beds and it was found to be statistically significant which was due to the increased number of patients per day. Although opposing observations were made by Patwary et al., 2009 who conducted waste generation study in private and government hospitals and small clinics of Dhaka city and found that small clinics with less number of patients generated more amount of waste. The opposite trend was mainly attributed to socio-economic and cultural condition and living standards of the patients and this may be also associated with more comfortable residential care and an increase number of tests per patient as observed by Rehman et al., 2007. However at government hospitals provide health services to poor patients that have relatively less socioeconomic status therefore small numbers of tests were usually prescribed to patients that may have resulted in generation of less amount of infectious and pathological waste instead of general waste which was observed in high quantity compared to any other hospital surveyed in this study.
Segregation of hospital waste is considered very important to enable proper waste disposal system. The current study revealed that 80% of the surveyed hospitals segregate hazardous waste from the non-hazardous waste at the source and store their waste in separate plastic bags and containers. The reason for waste segregation is to reduce the waste volume and responsibility to clean the environment. Without source segregation and recycling activities in place hospitals are supposed to dispose general waste along with infectious waste thereby resulting in unwanted disposal cost (Ananth et al., 2010). Proper segregation of waste is necessary to reduce the waste volume that needs special attention (Lee et al., 2004). A research was conducted in Bahrain and waste segregation practices were observed in 86 % of the hospitals by Mohamed et al., 2009.
Almost all the hospitals surveyed uses color coded bags which is an indication of efficient segregation practices. Similar type of research was conducted by Askarian et al., 2004 in which they reported that waste segregation is not conducted according to specific rules and regulations and hazardous waste is stored along with domestic waste which is due to lack of comprehensive staff training and to a lesser extent due to lack of facilities and this may probably is considered important factor for waste segregation. Since government hospital workers have more chances to participate in training that is why segregation was adapted as usual practice in these hospitals.
We found that medical staff of the government hospitals had better knowledge regarding waste management then private hospitals mainly due to higher percentage of training programes conducted in the former. It is generally agreed that hospital waste management can be enhanced considerably if appropriate training is given to hospital employees (Mohee et al., 2005) and it also reflects the better understanding of waste management policy of a concerned hospital (Ruoyan et al., 2010). Current study revealed that government hospitals have relatively clear defined waste management policies since 70 % hospitals provide training to staff regarding waste management and 85 % provide immunization protocol. Here importance of senior staff members in training programe cannot be denied because it has too advantages firstly this encourages young medical staff to acquire waste handling knowledge during training and secondly senior nurses, waste handlers and other related staff had better understanding of waste management and can comply to safety guidelines in a better way (Lymer et al., 2004). The effectiveness of such training programs lie in continuity and updation which is more followed in developed countries (Askarian et al., 2004) and also how frequently these are arranged (Birpinar et al., 2009; Abdullah et al., 2008). It is concluded that hospitals should provide sufficient training programs and protective measures to all relevant personnel involved in waste management in terms of occupational safety and education. To minimize the risk associated with hospital waste it seems training of senior and junior staff members regarding waste management is imperative. Government hospitals are more following that approach therefore hazards associated with hospital waste is comparatively less then private although in the former huge amount of waste is produced as compared to latter. However matter of concern emerged in this study is handling of pathological and sharp waste in private hospitals which require proper handling and disposal. It is therefore recommended that specific training pertaining to handling and disposal of such waste should be provided to medical staff of private hospitals. In this context ministry of health at federal and provincial level can play key role by instructing the hospital administration by providing proper manual and guidelines regarding waste management.
5. Conclusion
In this paper existing waste management techniques have been investigated to determine appropriate technology for waste management in the surveyed hospitals. It is revealed that the numbers of private and government hospitals throughout Rawalpindi are constantly increasing. This leads to an increase in the quantity of hazardous waste generated. The study depicted that segregation procedures of the different types of wastes were followed in 80 percent of the hospitals while in 20 percent of the hospitals waste segregation procedures were not followed consistently. Mostly infectious and non-infectious waste are mixed together before they properly disposed of due to i) lack of awareness of hospital staff ii) lack of skilled staff in waste management team. Therefore, it is recommended from the current study that source segregation of the waste, handling and transport, treatment and disposal are the basic elements of a management strategy that need to be outlined and regulated. Study indicated a need of training programs for different level of hospital staff from administrators and top managers to doctors and nurses, down to waste handlers and maintenance staff.
References
- Abdullah F, Qdais HA, Rabi A (2008) Site investigation on medical waste management practices in Northern Jordan. Waste Manage 28: 450-458
- Alagoz AZ, Kocasoy G (2008) Determination of the best appropriate management methods for the health-care wastes in Istanbul .Waste Manage 28: 1227–1235
- Ananth AGP, Prashanthini V, Visvanathan C (2010) Healthcare waste management in Asia. Waste Manage 30: 154-160
- Askarian M, Vainly M, Kabir G (2004) Results of hospital waste survey in private hospitals in Fars province, Iran. Waste Manage 24: 347-352
- Beveja G, Muralidhar S, Aggarwal P (2009) Medical waste management –an overview. Hospital today (5)9: 485-486
- Birpinar ME, Bilgili MS, Erdogan T (2009) Medical waste management in Turkey. Waste Manage 29: 445-448
- Chaerul M, Tanaka MA, Shekdar V (2008) A system dynamics approach for hospital waste management. Waste Manage 28: 442-449
- Coker A, Sangodoyin A, Sridhar M. Booth C, Olomolaiye P (2009) Medical waste management in Ibadan, Nigeria. Waste Manage 29: 809-811
- Diaz, LF, Eggerth LL, Enkhtsetseg S, Savage GM (2008) Characteristics of healthcare wastes. Waste Manage 28: 1219-1226
- Lee KB, Ellenbecker MJ, Eraso RM (2004) Alternatives for treatment and disposal cost reduction of regulated medical wastes. Waste Manage 24: 143–151
- Li J, Bai Q, Nie Y (2002) Future solutions for the treatment and disposal of hazardous wastes in China. Environ Manage 21: 591–597
- Lymer B, Richt B, Isaksson T (2004) Factors promoting health care workers compliance with guidelines in connection with risk. Journal of Clinical Nursing 13: 547-554
- Marinkovic N, Vitale K, Holcer NJ, Dzakula A, Pavic T (2008) Management of hazardous waste in Croatia. Waste Manage 28:1219-1226
- Mohamed LF, Ebharim SA, Al-Thukair AA (2009) Hazardous healthcare waste management in the kingdom of Bahrain. Waste Manage 29: 2402-2409
- Mohee R (2005) Medical waste characterization in healthcare institution in Mauritius. Waste Manage 25: 575-581
- Patwary MA, Hare WO, Street G, Elahi KM, Hossain SS, Sarker MH (2009) Quantitative assessment of medical waste generation in the capital city of Bangladesh. Waste Manage 29: 2392-2397
- Palenik CJ, Cumberlander ND (1993) Effects of steam sterilization on contents of sharp containers. American J Infectious Control 21: 28–33
- Ramasamy S, CJ Kumanan, K. Palanivel. 2003. GIS based solutions for waste disposal. In: GIS Development, India.
- Ruoyan G, Lingzhong X, Huijuan L, Chengchao Z, Jiangjiang H, Yoshihisa S, Wei T, Chuski K( 2010) Invertigation of health care waste management in Binzhou District, China. Waste Manage 30: 246-250
- Shinee E, Gombojav E, Nishimura A, Hamajima N (2008) Healthcare waste management in the capital city of Mongolia. Waste Manage 28: 435-441
- Silva CE, Hoppe AE, Ravanello MM, Mello N (2005) Medical waste management in South of Brazil. Waste Manage 25: 600-610
- Taghipour H, Mosaferi M (2008) Characterization of medical waste from hospitals in Tabriz, Iran. Sci. Total Environ 5: 1527-1535
- Tudor TL, Noonan CL, Jenkin LET (2005) Healthcare waste management: a case study from the National Health Service in Cornwall, United Kingdom. WasteManage 25: 606–615
- Yong Z, Gang X, Guanxing W, Tao Z, Dawei J (2009) Medical waste management in China: A case study of Nanjing. Waste Manage 29: 1376-1382



